Read Pediatric Primary Care Case Studies Online
Authors: Catherine E. Burns,Beth Richardson,Cpnp Rn Dns Beth Richardson,Margaret Brady
Tags: #Medical, #Health Care Delivery, #Nursing, #Pediatric & Neonatal, #Pediatrics
Pediatric Primary Care Case Studies (60 page)

Maya’s mother reports giving Advil at an appropriate dosage (10 mg/kg/dose) every 6 hours for the persistent fever. She denies the use of any other alternative medication. The child feels worse than she did 3 days ago despite the Advil and the Omnicef. The mother reports that Maya is usually very energetic, and her present behavior is unusual. The mother also denies any history of high persistent fever(s) or serious illnesses in the past.
Due to the lack of response to antibiotic and the presence of lymphadenopathy, fatigue, persistent fever, and tonsillitis, you consider infections such as infectious mononucleosis (IM), which would include signs and symptoms such as Maya’s that do not improve with antibiotic treatment.
What other questions do you need to ask Maya and her mother?

Before answering this question, here is some background information about pharyngitis and infectious mononucleosis (IM) that may be helpful to you. Pharyngitis is the third most common complaint in pediatric primary care settings. In this case, the complaint is more complex than a simple pharyngitis and points in the direction of IM with a secondary group A streptococcus infection. You need to consider the pathophysiology, epidemiology, differential diagnosis, and cultural factors before answering this question.
Pathophysiology of Infectious Mononucleosis
A sore throat presents with pain localized to the pharynx, surrounding anatomy, and the neck and is accompanied by dysphasia. The younger the child, the greater the difficulty in identifying the area of painful symptoms. A history of
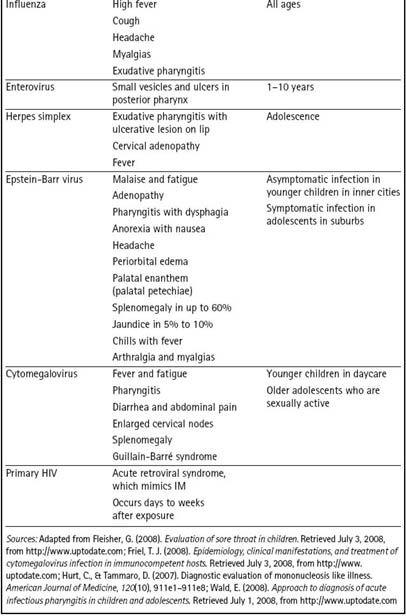
fever and decreased oral intake is one of the signs of pharyngitis in a nontoxic child. There may be accompanying fever, pharyngeal exudates, tonsillar enlargement, uvula inflammation, headache, palatal petechiae, ulcers of the tonsillar pillars, and soft palate, along with anterior cervical lymph node enlargement (Bisno, Gerber, Gwalty, Kaplan, & Schwartz, 2002). The etiology with acute infectious pharyngitis includes bacteria and viruses (see
Table 16-1
).
IM varies from a simple pharyngitis in that the course is prolonged with fever, lymphadenopathy, and fatigue. Epstein-Barr virus (EBV) is responsible for up to 90% of infectious mononucleosis in adolescent and adults (Hurt & Tammaro, 2007); however, in younger children, the infection is generally sub-clinical (Hurt & Tammaro; Rezk & Weiss, 2007). The term
IM
indicates a constellation of symptoms that arises from infection with a host of viruses including EBV; however, 10% of IM-like pediatric cases are caused by cytomegalovirus (CMV), human immunodeficiency virus (HIV), or toxoplasmosis infection (Hurt & Tammaro; Smellie et al., 2007). Thus, although the majority of cases of IM are from EBV, other causes need to be considered.
EBV infects the B lymphocytes of the lymphoid-rich areas of the oropharynx, which disseminate the infection in the lymphoreticular system (Rezk & Weiss, 2007). This predilection of EBV to entrench itself within the lymphoreticular system allows for a reservoir of EBV within the B-cells and causes its persistence. The persistence of EBV genes in B-cells results in viral latency and a carrier state (Rezk & Weiss). In addition, EBV-specific cytotoxic T-cell lymphocytes control acute infection and reactivation of infection (Kimura, 2006). This T-cell activation causes production of interleukin 2 and cytokines, causing atypical lymphocytes to appear on a complete blood count (Kimura). The clinical illness of IM may reflect cell damage in the oropharynx caused by viral replication, B-cell proliferation with a rise in cytokine levels, and immunopathology due to the immune response to the virus (Vetsika & Callan, 2004).
CMV has the largest genome size of any virus that infects humans and is a member of the human herpes virus. Human herpes viruses all establish viral latency in the cells they infect; thus, they can reoccur or shed intermittently (Adler & Marshall, 2007). The inner core of viral DNA is contained in a capsid surrounded by a tegument layer and an outer layer composed of glycoproteins. The antigenic glycoproteins trigger an immune response, which includes T-cells (Adler & Marshall). CMV viral DNA can be found in megakaryocytes, monocytes, dendritic cells, and myeloid progenitor cells (Soderberg-Naucler et al., 2001). Reactivation is more likely to occur when the human host is immunosuppressed. Incubation is estimated to be between 1 and 2 months (Adler & Marshall).
Acute infection with HIV was first described as a monolike illness in 1985 (Cooper et al., 1985). After a period of incubation of 2–4 weeks following an acute infection, patients can develop sore throat, malaise, myalgias, arthralgias, nausea, and headache. A nonpruritic maculopapular rash can also be seen (Hurt & Tammaro, 2007).
Toxoplasmosis is the main protozoal cause of a mononucleosis-like illness that can present with rather mild constitutional symptoms of pharyngitis,
maculopapular rashes, nontender cervical or occipital lymphadenopathy, and hepatosplenomegaly. This is a self-limited illness and resolves spontaneously over a few months.
Table 16–1 Common Infectious Agents and Acute Pharyngitis

Epidemiology
EBV is transmitted via saliva between individuals and has an incubation period of 4–7 weeks (Vetsika & Callan, 2004). After incubation, pharyngitis, lymphadenopathy, splenomegaly, and fatigue occur. The elevation of transaminases (SGPT, SGOT), indicating a hepatitis, may be evident but jaundice is present in less than 10% of patients (Vetsika & Callan).
CMV is excreted in nearly all body secretions except tears (Adler & Marshall, 2007). Transfusion of CMV-infected blood into a CMV-negative person can cause CMV infection and has been rarely reported as a result of nosocomial contact within a hospital. CMV-caused IM (CMV IM) in children, adolescents, and adults can occur in situations involving close contact with children under age 2 years. Daycare workers and school teachers are at higher risk (Hurt & Tammaro, 2007). Whereas sore throat, fatigue, and malaise are prominent features of IM, CMV IM presents with less prominent lymphadenopathy, pharyngeal erythema, and splenomegaly. Elevated transaminases occur much more commonly with CMV IM.
Toxoplasmosis is found throughout the world, and the members of the cat family are the host. Cats get the infection from eating mice or uncooked meat. The cat sheds the oocyst 3 to 30 days after the ingestion. Transmission also can occur through transfusion or transplantation. Mothers can also transmit the infection to their unborn children. The clinical presentation after the newborn period includes fever, sore throat, lymphadenopathy, and malaise (Pickering, Baker, Long, & McMillan, 2006).
Cultural and Ethnic Aspects
The Hispanic American population is the second largest and fastest-growing population in the United States. To deliver culturally effective pediatric care, the provider needs to understand the beliefs, values, and customs of the population (American Academy of Pediatrics, Committee on Pediatric Workforce, 2004). Flores (2000) identified five normative cultural values that are highly valued by Hispanics and are important to consider in interpersonal interactions:
•
Simpatia
, or kindness expressed to family in times of stress
•
Personalismo
, or formal friendliness
•
Respeto
, or admiration
•
Familismo
, or loyalty to family
•
Fatalsimo
, or the belief that fate cannot be altered
In addition, some Hispanic cultures believe in the “hot–cold” theory and others believe in subtle variations of this theory (Hardwood, 1971). The hot–cold theory
of illness is centered on the belief that the body reacts to heat and cold. Some illnesses, often including symptoms of redness or swelling, are classified as hot. Other illnesses such as respiratory infections are cold. Cold illnesses require hot remedies, and hot illnesses are treated with cold foods.
In caring for this family, the provider needs to determine how the parent’s ethnic beliefs would affect the care of the child. It is important to show respect for the mother’s culture and country as well as formal friendliness by introduction as a primary care provider. It is essential to give an appropriate amount of simpatico about her daughter’s illness.
The mother thinks of herself as more American than Puerto Rican and denies belief in the hot–cold theory of disease.
Differential Diagnosis
The oncological differential diagnosis for infectious mononucleosis includes acute leukemia, Hodgkin’s disease, non-Hodgkin’s lymphoma, and solid tumors of the neck. The differential diagnosis for pharyngitis includes bacterial, viral, and protozoal causes (see
Table 16-1
). Many infectious agents have seasonal prevalence, and some infectious agents are more common in different age groups. Allergies can also cause throat pain or pharyngeal tickling, but would not be accompanied by a fever. Acute sinusitis could present with fever, headache, pharyngitis, and cervical adenopathy, but frequently presents with congestion and purulent nasal discharge.
History
From the above review, what other information do you need to obtain?
• Are other family members ill or have they been ill in the past 2–3 months?
• Have close friends been ill in the past 2–3 months? (exposure to infectious diseases)
• Is the child in the after-school program involved with the children in the daycare? (exposure to CMV)
• Is the child taking any medication for health? (explores alternative medication use)
• Has the child been in school over the past week? (confirms fatigue and nature of illness)