The Theory and Practice of Group Psychotherapy (47 page)
Read The Theory and Practice of Group Psychotherapy Online
Authors: Irvin D. Yalom,Molyn Leszcz
Tags: #Psychology, #General, #Psychotherapy, #Group

Good attendance is so necessary for the development of a cohesive group that it is wise to exclude clients who, for any reason, may not attend regularly. Poor attendance may be due to unpredictable and hard-to-control work demands, or it may be an expression of initial resistance to therapy. I do not select individuals whose work requires extensive travel that would cause them to miss even one out of every four or five meetings. Similarly, I am hesitant to select clients who must depend on others for transportation to the group or who would have a very long commute to the group. Too often, especially early in the course of a group, a client may feel neglected or dissatisfied with a meeting, perhaps because another member may have received the bulk of the group time and attention, or the group may have been busy building its own infrastructure—work that may not offer obvious immediate gratification. Deep feelings of frustration may, if coupled with a long, strenuous commute, dampen motivation and result in sporadic attendance.
Obviously, there are many exceptions: some therapists tell of clients who faithfully fly to meetings from remote regions month after month. As a general rule, however, the therapist does well to heed this factor. For clients who live at considerable distance and have equivalent groups elsewhere, it is in everyone’s interests to refer them to a group closer to home.
These clinical criteria for exclusion are broad and crude. Some therapists have attempted to arrive at more refined criteria through systematic study of clients who have failed to derive benefit from group therapy. Let me examine the research on one category of unsuccessful clients: the group therapy dropouts.
Dropouts
There is evidence that premature termination from group therapy is bad for the client and bad for the group. In a study of thirty-five clients who dropped out of long-term heterogeneous interactional outpatient groups in twelve or fewer meetings, I found that only three reported themselves as improved.
22
Moreover, those three individuals had only marginal symptomatic improvement. None of the thirty-five clients left therapy because they had satisfactorily concluded their work; they had all been dissatisfied with the therapy group experience. Their premature terminations had, in addition, an adverse effect on the remaining members of the group, who were threatened and demoralized by the early dropouts. In fact, many group leaders report a “wave effect,” with dropouts begetting other dropouts. The proper development of a group requires membership stability; a rash of dropouts may delay the maturation of a group for months.
Early group termination is thus a failure for the individual and a detriment to the therapy of the remainder of the group. Unfortunately, it is common across the psychotherapies. A recent empirical analysis concluded that 47 percent of all clients leave psychotherapy (group and individual therapy as well) prematurely.
23
Even in expert hands some dropouts are unavoidable, no doubt because of the complex interplay of client, group, and therapist variables.
24
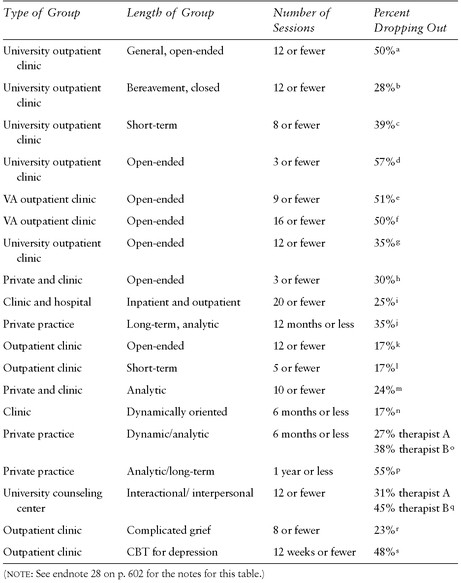
Consider the dropout rates displayed in
table 8.1
: group therapy attrition ranges from 17 percent to 57 percent. Although this rate is no higher than the dropout rate from individual therapy, the dropout phenomenon is of more concern to group therapists because of the deleterious effects of dropouts on the rest of the group.
A study of early dropouts may help establish sound exclusion criteria and, furthermore, may provide an important goal for the selection process. If, in the selection process, we learn merely to screen out members destined to drop out of therapy,
that in itself
would constitute a major achievement. Although the early terminators are not the only failures in group therapy, they are unequivocal failures.† We may, I think, dismiss as unlikely the possibility that early dropouts will have gained something positive that will manifest itself later. A relevant outcome study of encounter group participants noted that individuals who had a negative experience in the group did not, when studied six months later, “put it all together” and enjoy a delayed benefit from the group experience.
25
If they left the group shaken or discouraged, they were very likely to remain that way. (One exception to the rule may be individuals who enter in some urgent life crisis and terminate therapy as soon as the crisis is resolved.)
Keep in mind that the study of group dropouts tells us little about the group continuers; group continuation is a necessary but insufficient factor in successful therapy, although evidence exists that clients who continue in treatment and avoid premature or forced ending achieve the best therapy outcomes.
26
Reasons for Premature Termination
A number of rigorous studies of group therapy in various settings (ambulatory, day hospital, Veterans Administration clinics, and private practice, including both heterogeneous groups and homogeneous groups for problems such as grief or depression, and conducted in an interactional manner or along cognitive-behavioral lines) have convergent findings.
27
,
28
These studies demonstrate that clients who drop out prematurely from group therapy are likely, at the initial screening or in the first few meetings, to have one or more of the following characteristics:
• Lower psychological-mindedness
• Reduced capacity to think about emotions without action
• Lower motivation
• More reactive than reflective
• Less positive emotion
• Greater denial
• Higher somatization
• Abuse of substances
• Greater anger and hostility
• Lower socioeconomic class and social effectiveness
• Lower intelligence
• Lack of understanding of how group therapy works
• The experience or expectation of cultural insensitivity
• Less likable (at least according to therapists)
TABLE 8.1
Group Therapy Dropout Rates
These conclusions suggest that, unfortunately, the rich get richer and the poor get poorer. What a paradox! The clients who have the least skills and attributes needed for working in a group—
the very ones who most need what the group has to offer
—are those most likely to fail! It is this paradox (along with economic issues) that has stimulated attempts to modify the therapy group experience sufficiently with different structures and outreach to accommodate more of these at-risk clients.†
Keep in mind that these characteristics should therefore be seen as cautions rather than absolute contraindications. The person who fails in one group or in one type of group may do well in a different one. We should aim to reduce, not eliminate dropouts. If we create groups that never experience a dropout, then it may be that we are setting our bar for entry too high, thus eliminating clients in need who we may in fact be able to help.
I will discuss one final study here in great detail, since it has considerable relevance for the selection process.
29
I studied the first six months of nine therapy groups in a university outpatient clinic and investigated all clients who terminated in twelve or fewer meetings. A total of ninety-seven clients were involved in these groups (seventy-one original members and twenty-six later additions); of these, thirty-five were early dropouts. Considerable data were generated from interviews and questionnaire studies of the dropouts and their therapists as well as from the records and observations of the group sessions and historical and demographic data from the case records.
An analysis of the data suggested nine major reasons for the clients’ dropping out of therapy:
1. External factors
2. Group deviancy
3. Problems of intimacy
4. Fear of emotional contagion
5. Inability to share the therapist
6. Complications of concurrent individual and group therapy
7. Early provocateurs
8. Inadequate orientation to therapy
9. Complications arising from subgrouping
Usually more than one factor is involved in the decision to terminate. Some factors are more closely related to external circumstances or to enduring character traits that the client brings to the group, and thus are relevant to the selection process, whereas others are related to the therapist or to problems arising within the group (for example, the therapist’s skill and competence, client-therapist interaction variables, and the group culture itself)† and thus are more relevant to therapist technique (I will discuss these issues in chapters 10 and 11). Most relevant to the establishment of selection criteria are the clients who dropped out because of
external factors, group deviancy, and problems of intimacy
.
External Factors.
Logistical
reasons
for terminating therapy (for example, irreconcilable scheduling conflicts, moving out of the geographic area) played a negligible role in decisions to terminate. When this reason was offered by the client, closer study usually revealed group-related stress that was more pertinent to the client’s departure. Nevertheless, in the initial screening session, the therapist should always inquire about any pending major life changes, such as a move. There is considerable evidence that therapy aimed at both symptom relief and making major changes in the clients’ underlying character structure is not a brief form of therapy—a minimum of six months is necessary†—and that clients should not be accepted into such therapy if there is a considerable likelihood of forced termination within the next few months. Such individuals are better candidates for shorter-term, problem-oriented groups.
External stress
was considered a factor in the premature dropout of several clients who were so disturbed by external events in their lives that it was difficult for them to expend the energy for involvement in the group. They could not explore their relationships with other group members while they were consumed with the threat of disruption of relationships with the most significant people in their lives. It seemed especially pointless and frustrating to them to hear other group members discuss their problems when their own problems seemed so compelling. Among the external stresses were severe marital discord with impending divorce, impending career or academic failure, disruptive relationship with family members, bereavement, and severe physical illness. In such instances referrals should be made to groups explicitly designed to deal with such situations: acute grief, for example, is generally a time-limited condition, and the acutely bereaved client is best referred to a short-term bereavement group.
30
Note an important difference! If the goal is specifically (and nothing more than) to get rid of the pain of a break up, then a brief, problem-oriented therapy is indicated. But if the client wishes to change something in himself that causes him to thrust himself repetitively into such painful situations (for example, he continues to become involved with women who invariably leave him), then longer-term group work is indicated.
The importance of external stress
as a factor in premature group termination was difficult to gauge, since often it appeared secondary to internal forces. A client’s psychic turmoil may cause disruption of his or her life situation so that secondary external stress occurs; or a client may focus on an external problem, magnifying it as a means of escaping anxiety originating from the group therapy. Several clients considered external stress the chief reason for termination; but in each instance, careful study suggested that external stress was at best a contributory but not sufficient cause for the dropout. Undue focusing on external events often seemed to be one manifestation of a denial mechanism that was helping the client avoid something perceived as dangerous in the group.
In the selection process, therefore, consider an unwarranted focusing on external stress an unfavorable sign for intensive group therapy, whether it represents an extraordinary amount of stress or a manifestation of denial.
Group Deviancy.
The study of clients who drop out of therapy because they are group deviants offers a rich supply of information relevant to the selection process. But first the term
deviant
must be carefully defined. Almost every group member is deviant in the sense of representing an extreme in at least one dimension—for example, the youngest member, the only unmarried member, the sickest, the only Asian-American, the only student, the angriest, the quietest.