Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis (157 page)
Authors: Mary A. Williamson Mt(ascp) Phd,L. Michael Snyder Md

BOOK: Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis
6.59Mb size Format: txt, pdf, ePub
The patient may present with stigmata of chronic blood loss (
iron deficiency
anemia and related symptoms) or acute blood loss (weakness or syncope).
Screening
: Currently, screening for asymptomatic ulcerated lesions of the GI tract is generally recommended, especially for carcinoma of the colon and large adenomas.
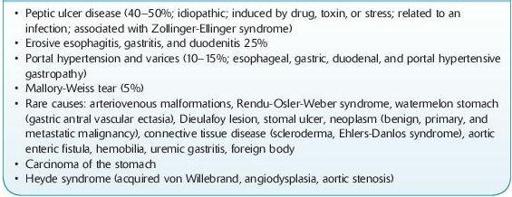
Differential Diagnosis of Upper Gastrointestinal Bleeding (Table
5-3
)
PUD (see discussion of acute abdomen under Abdominal Pain) (40–50% of patients) is associated with risk factors including
H. pylori
infection, use of NSAIDs, stress, and increase of gastric acid. It accounts for gastritis in 10% of patients, esophagitis 6% associated with gastric reflux (GERD). Risk factors for stress-related bleeding include respiratory failure and coagulopathy. Portal hypertension and varices (18% of patients) indicate the severity of a patient’s underlying cirrhosis. These patients have an associated mortality of 50% even after control of the hemorrhage.
TABLE 5–3. Differential Diagnosis of Upper Gastrointestinal Bleeding
Other books
The Dulcimer Boy by Tor Seidler
When We Were Sisters by Emilie Richards
The River of Wind by Kathryn Lasky
Clochemerle by Gabriel Chevallier
Eldritch Manor by Kim Thompson
There's a Man With a Gun Over There by R. M. Ryan
Strangers From the Sky by Margaret Wander Bonanno
Dangerous Love by Walters, Ednah, Walters, E. B.
Hung Out: A Needles and Pins Rock Romance by Creed, Lyrica
Hungry Heart: Konigsburg, Texas, Book 8 by Meg Benjamin