Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis (543 page)
Authors: Mary A. Williamson Mt(ascp) Phd,L. Michael Snyder Md

BOOK: Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis
7.71Mb size Format: txt, pdf, ePub
Focal nephritic: generally associated with inflammatory regions in less than one half of glomeruli. Patients often present with asymptomatic hematuria and proteinuria.
Causes
Renal: can be postinfectious (due to certain nephritogenic strains after streptococcal, staphylococcal, or pneumococcal infections, mumps, measles, chickenpox, hepatitis B and C) or due to MPGN or anti–glomerular membrane disease.
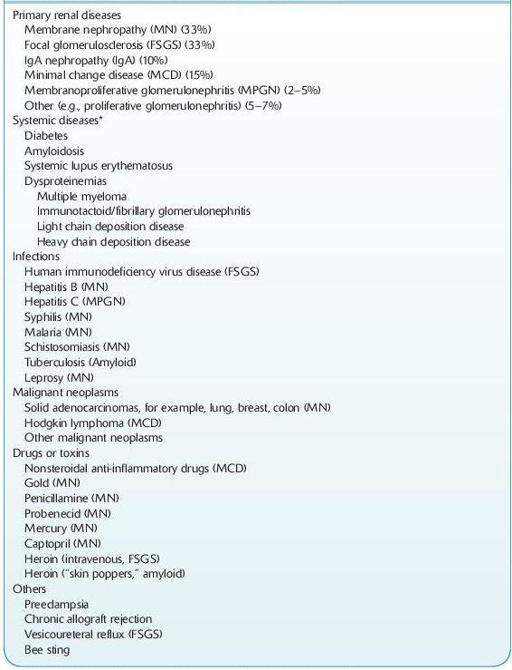
NEPHROTIC SYNDROME
This syndrome presents as heavy proteinuria, hypoalbuminemia, hyperlipidemia, lipiduria, and edema.
12-5
).
TABLE 12–5. Major causes of Nephrotic Syndrome
Other books
War Baby by Colin Falconer
Primal Claim by Marie Johnston
Promise Cove (A Pelican Pointe Novel Book 1) by Vickie McKeehan
Where the Road Takes Me by Jay McLean
Alpha Wolf's Calling by Hannah Heat
No New Land by M.G. Vassanji
The Reckoning on Cane Hill: A Novel by Steve Mosby
Gifted Stone by Kelly Walker
First Times: Nine Tales of Innocence Lost by Natalie Deschain
Lucan: The Pendragon Legacy by Susan Kearney