i bc27f85be50b71b1 (84 page)
Read i bc27f85be50b71b1 Online
Authors: Unknown



NERVOUS SYSTEM
281
•
Does the pariem have an altered sleep pattern?
•
What is the handedness of the patient? (Handedness is a predicror of brain [language] dominance.)
Observation
Data that can be gathered from close or distant observation of the
patient include the following:
•
Level of alertness, arousal, distress, or the need for restraint
•
Body position
•
Head, trunk, and extremity posture, including movement patterns
•
Amount and quality of active movement
•
Amount and quality of interaction with the environment or
family members
•
Degree of ease or difficulty with activities of daily living
•
Presence of involuntary movements, such as tremor
•
Eye movement(s)
•
Presence of hemibody or hemispace neglect
•
Presence of muscle atrophy
•
Respiratory rate and pattern
Clinical Tip
The therapist should correlate these observations with
other information from the chart review and other health
care team members ro determine (1) if the diagnosis is consistent with the physical presentation, (2) what rypes of
commands or tone of voice to use, (3) how much assistance is needed, and (4) how to prioritize the portions of the physical therapy evaluation.

282 AClITE CARE HANDBOOK FOR PHYSICAL THERAPISTS
Mental Status Exam;natioll
The mental status examination includes assessment of level of consciousness, cognition, emotional state, and speech and language ability.
Level of Consciousness
COlIsc;ouslless consists of arousal and the awareness of self and
environment, including the ability to interact appropriately in
response to any normal stimulus' Coma is often considered the
opposite of consciousness. Table 4- 1 0 describes the different States
of consciousness. Evaluating a patient's level of consciollsness is
important because it serves as a baseline ro monitor stability,
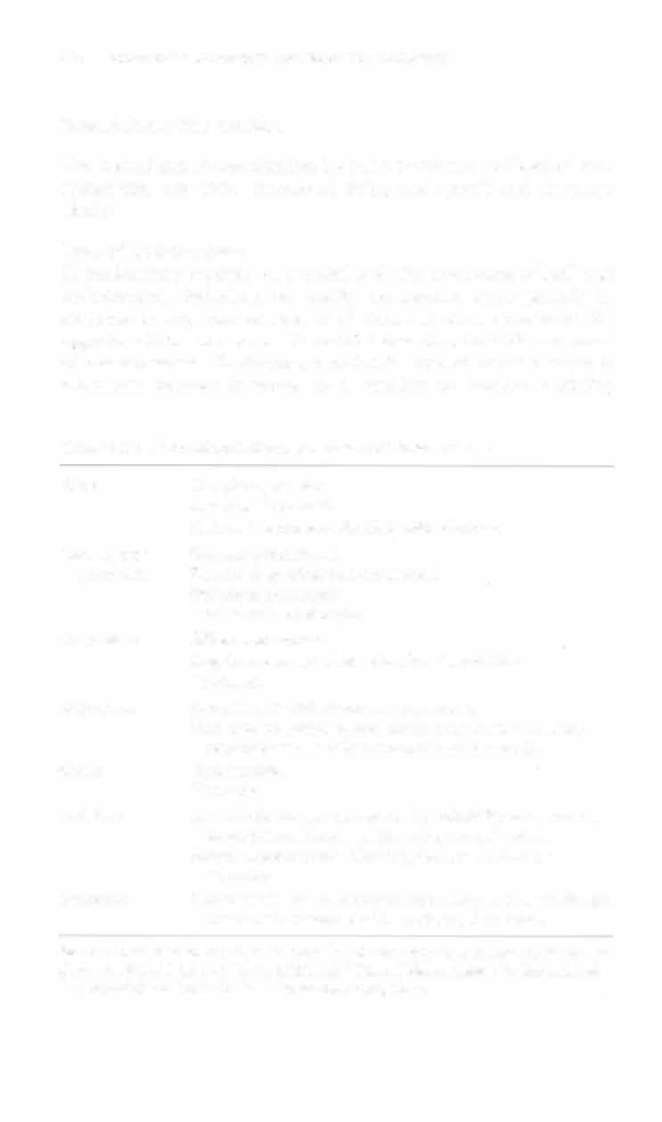
Table 4-10. Normal and Abnormal States of Consciousness
Alerr
Completely awake.
Aware of all stimuli.
Able to interact meaningfully with clinician.
Lethargic or
Arousal with stimuli.
somnolent
Falls to sleep when nor stimulared.
Decreased awareness.
Loss of train of thought.
Obtundent
Difficult to arouse.
Requires constant stimulation for all activities.
Confused.
Stuporous
Arousal only with vigorous stimulation.
Unable to complete mental Status examination because
responses are usually incomprehensible words.
Coma
Unarousable.
Nonverbal.
Delirium
State of disorientation marked by irritability or agitation,
suspicion and fear, and misperception of stimuli.
Patient demonstrates offensive, loud, and talkative
behaviors.
Dementia
Alteration in mental processes secondary to organic disease
that is nor accompanied by a change in arousal.
Sources: Data from RL Strub, FW Black (cds). Mcntal Status Examination in Neurolo!,'Y
(2nd cd). Philadelphia: FA Davis, 1985; and F Plum, J Posner (cds). The Diagnosis of
Scupor and Coma (3rd cd). Phil3delphia: FA Davis, 1980.


NERVOUS SYSTEM 283
improvement, or decline in the patient's condition. It also helps
determine the severity and prognosis of neurologic insult or disease state, thus directing the medical plan of care.
Clinical Tip
•
Level of consciousness is often vaguely described in
medical charts; therefore, be specific when documenting
a patient's mental status. Describe [he intensity of stimulus needed to arouse the patient, the patient's best
response, and the patient's response to the removal of
the srimulus.9
•
Changes in body position, especially the transition from
a recumbent position to sitting upright, often stimulate
increased alertness. Other stimuli to increase alertness
include daylight, radio or television sound, or a cold cloth
on the forehead.
•
Use a progressive intensity of stimuli to arouse a patient
with decreased alertness or level of consciollsness. For
example, call the patient's name in a normal tone of voice
before using a loud tone of voice, or tap the patient'S
shoulder before rubbing the shoulder.
• Time of day, fatigue, and side effects of medication
are factors that can calise variable levels of alertness or
participation in physical therapy. The documentation of
these factors is important for communication among the
health care team and for the rehabilitation screening
process.
•
A & 0 x 3 is a common abbreviation for alert and
oriented to person, place, and time. The number may be
modified to reflect the patient'S orientation (e.g., A & 0
x I [selfl).
Glasgow Coma Scale
The Glasgow Coma Scale (GCS) is a widely accepted measure of level
of consciousness and responsiveness and is described in Table 4-:1 1 .
The GCS evaluates best eye opening (E), motor response (M), and
verbal response (V). To determine a patient'S overall GCS, add each