Murder and Mayhem (13 page)
Authors: D P Lyle

Certain chemicals may artificially produce similar reactions.
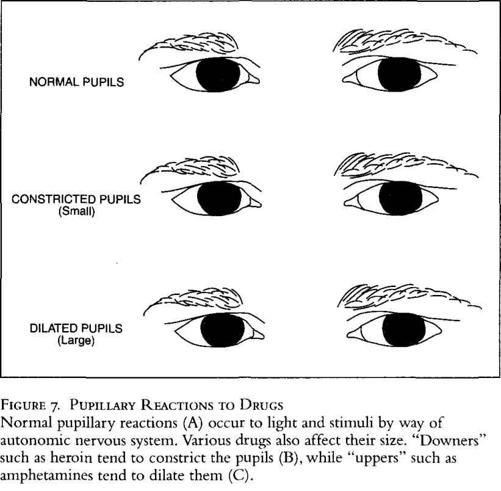
"Downers" such as narcotics tend to relax and stupefy (no pun intended) and thus constrict the pupils. These include drugs such as heroin, morphine, and barbiturates. "Uppers," or speedlike compounds, are classified as sympathomimetic drugs since they mimic the effect of the sympathetic portion of the ANS. They tend to dilate the pupils. Cocaine, amphetamines, crystal methampheta-mine, Ecstasy, and many diet pills do this. Marijuana also tends to enlarge the pupils.
How Safe Is It to Handle Cyanide?
Q: What would happen if a person handling cyanide didn't wear gloves but had limited contact with it?
A: Obviously, what happens is dependent on what exposure occurred, the concentration of the cyanide handled, and the point of exposure. But cyanide is a toxic and very dangerous substance.
Cyanide can absorb directly through the skin and kill you. Gloves would prevent that. If the powder is shaken into the air and inhaled, it will enter the bloodstream rapidly via the lungs and kill you. If it is dissolved in a liquid and the liquid is spilled on the skin or splashed in the eyes, it will kill you.
It takes only a small amount, and even if a doctor was standing right next to you, you would still die.
Bad stuff. Unless you want your character to kill someone, then it's great. But there is no such thing as too much caution when handling it.
Will Food Intake Prevent Alcohol Intoxication?
Q: My character is in a situation where she must drink considerably while minimizing the effects of intoxication. Is there a substance that one can inject or ingest to combat alcohol intoxication (prior to consuming the alcohol)? What about the old adage that a significant quantity of bread will "absorb" the alcohol?
A: Ingested alcohol is absorbed into the bloodstream very rapidly, and as soon as the blood passes through the liver, the liver begins to extract it from the blood and break it down. The level of alcohol in the blood at any given time is a dynamic balance between the rate of absorption from the gastrointestinal (GI) tract and the rate of destruction and elimination by the liver.
Bread does not absorb or soak up alcohol. But any food in the stomach, including bread, will slow the passage of alcohol into the bloodstream and thus lower the blood alcohol level. Alcohol is
absorbed at all levels of the GI tract but enters the bloodstream faster from the small intestine, particularly the duodenum (the first part of the small intestine), than from the stomach. Fatty foods and milk tend to slow stomach emptying and thus would hold the alcohol in the stomach longer. The net effect is a slowing of alcohol absorption, so a cheeseburger and a milk shake might be a better pre-binge meal. Of course, drinking less and drinking slower makes the most sense for your character.
How Dangerous Is It to Transport Heroin in a Swallowed Condom?
Q: If you have a "mule" who has swallowed a condom full of heroin, how long before he passes it? How likely is the condom to succumb to digestive fluids and leak?
A: Normal gastrointestinal (GI) transit time (the time required to go from one end to the other—you get the idea) is twenty-four to seventy-two hours, a broad range. The actual transit time varies greatly from one person to another and from day to day in a given individual. In addition to this personal variability, it changes with age, the type of foods eaten recently, any GI diseases that might be present, any medications taken, the level of hydration, and a ton of other factors. Transit time is hard to predict.
That said, the mule would probably pass it in one to three days. Of course, the condoms are visible on an abdominal X ray, so if the customs officer or DEA agent suspects someone, he can easily find the contraband. He then gives laxatives to speed up the transit time and soon has the evidence in hand, so to speak.
The carriers use condoms or other latex, rubberlike containers because the body can't digest them easily, if at all. However, the acids and digestive enzymes found in the GI tract, coupled with the peristaltic motions of the intestines, can weaken a condom and
cause it to leak or break. In this circumstance death from absorption of the huge dose of cocaine, heroin, or other drug is typically quick and dramatic. Cocaine and methamphetamine cause seizures, cardiac arrhythmias, heart attacks, and death. Heroin causes a dramatic drop in blood pressure, suppression of respiration to the point of apnea (no breathing), and death.
Can Opium Addiction Make Someone Violent?
Q: I need help. One of my characters has found a hundred-year-old suicide letter. The writer says he has become addicted to opium, his personality has changed, he's become violent and nasty, and he intends to kill himself to keep from burdening his family. My writers' group questioned whether opium would make someone violent. If someone did become addicted to a substance in the late 1800s and had a personality change for the worse, what drug would it have been if not opium?
A: Opium, which is a gummy substance obtained from the opium poppy (
Papaver somniferium),
is a central nervous system depressant. It's the basis for morphine and heroin, and is a "downer." It causes lethargy and sleepiness, slow movements, depression, and in larger doses, coma and death. It is unlikely to stimulate violent or nasty behavior. That said, an opium addict who is undergoing withdrawal, either voluntary or forced, either jailed or unable to resup-ply himself, can become angry, aggressive, and even homicidal. So, yes, opium can indirectly cause the effects you want.
One other thought: In your scenario it is the letter writer who states that his own behavior has changed. Is that real or imagined? Is there corroboration of this statement from a more reliable source? He's an addict, so his assessment may not be accurate. Maybe he is having violent dreams or hallucinations that he
believes are true when in fact he is as gentle as a lamb—and depressed and suicidal. Opium can easily cause these types of delusions.
Another drug choice might be cocaine, which was available during the nineteenth century. Users often become aggressive, short-tempered, and violent. Chronic use can cause paranoia, which can feed the underlying aggressive behavior. This is probably a better choice if it fits your story.
Of course, he could have been addicted to both drugs. For a brief period of time during the nineteenth century, Sigmund Freud and others advocated cocaine as a treatment for opium addiction. Its stimulatory effects were seen as beneficial. After it became apparent that those treated in this manner became addicted to the cocaine, this treatment modality fell from favor. Perhaps the suicide letter or others found with it could mention that he had sought treatment for his addiction but was now despondent that the cure became its own curse.
Another possibility is alcohol, which is common and easily available. Alcoholics often become aggressive, nasty, and even homicidal. And suicidal.
Suicide is common among opium, cocaine, and alcohol abusers, as are accidental deaths from taking too much or combining drugs such as an opiate and alcohol. An interesting twist might be that the letter finder later acquires other evidence that indicate the suicide was perhaps not a serious attempt by the writer to take his own life but rather a gesture or cry for help that went too far. All too often addicts don't know how to ask for help, especially a hundred years ago, and believe that a suicide attempt will get them the attention they need.
Is Ritalin Useful in the Treatment of Attention Deficit Disorder; and How Can It Be Abused?
Q: My character's twelve-year-old son is put on Ritalin for attention deficit disorder. What would be the usual dose? How effective is it likely to be, and are there any side effects? Also, I read that this drug is commonly abused. How? By whom?
A: Attention deficit disorder (ADD) is not uncommon. It goes by several other names, such as hyperactive or hyperkinetic child syndrome and minimal brain dysfunction syndrome. The characteristic symptoms of this disorder are short attention span, distractibility, emotional lability, impulsive actions, and hyperactivity. Learning may or may not be impaired. The diagnosis of ADD is not straightforward and depends more on the presence of several of these symptoms rather than the results of any specific test. Neurologic exams, such as electroencephalograms (EEGs), MRIs, and CT brain scans, are most often normal.
Ritalin (methylphenidate hydrochloride) is effective for many sufferers of ADD. It is given orally twice per day, typically before breakfast and lunch. The typically recommended starting dose is 5 milligrams (mg) twice a day, which is increased by 5 to 10 mg every week until the desired effect is attained. The maximum dose should not exceed 60 mg per day. Ritalin comes in small round tablets of 5 mg (yellow), 10 mg (pale green), and 20 mg (pale yellow). There is also Ritalin SR (white), a 20-milligram sustained release tablet that is taken only once a day in the morning.
Ritalin may lessen or eliminate the symptoms of ADD. Alternatively, one of its many side effects may occur; these include rashes, loss of appetite, nausea, headache, drowsiness, an increase or decrease in blood pressure and pulse rate, palpitations, and even a toxic psychosis, in which delusions and hallucinations may occur.
Yes, Ritalin is a newcomer to the drug abuse crowd. It is ground and snorted and tends to give a rush similar to cocaine or metham-phetamine. Many primary schools have policies, stating that any medications taken by students during school hours must be given by the school nurse. The school bullies know this and watch to see which kids visit the nurse each morning to get their daily medications. Then they force the kids to hand them over and use the pills themselves or sell them to someone—kind of like a primary school Mafia.
It is also found in high schools and on college campuses. An unscrupulous doctor or pharmacist can often be found who will prescribe or dispense the drug. In addition, Ritalin is an overpre-scribed medication (meaning it is given to patients who don't really need it, much as Valium was in the past), and thus there is a lot of it out there on the streets. A ready supply and a growing demand means escalating abuse.
What
Is Seasickness?
Q: My novel is set in Victorian Boston. One of my characters, a middle-aged woman, must sail to England. She has severe seasickness every time she gets on a boat. What treatment might her physician suggest to get her through the trip?
A: There were many treatments for seasickness at that time, but none of them worked very well. One reason was that little was known of the physiology of this disorder. One popular theory postulated that it was caused by disturbances in the circulation of blood to the brain, which caused it to become anemic and thus produced nausea, vomiting, and dizziness, the major symptoms of motion sickness.
We now know that seasickness, motion sickness, and space sickness (due to weightlessness) are caused by scrambled signals received by the vestibular system (balance center) of the inner ear. As part of this elaborate system, the semicircular canals are the primary sensors of position and motion. They consist of three canals, each in a 90-degree plane to the other two, similar to the XYZ planes of solid geometry. One loops front and back, one right and left, and the last up and down. The canals are filled with fluid, and the action of gravity on this fluid lets the brain know if it is right side up, upside down, moving in a circle, and so forth.
In a weightless environment these signals are lost because there is no gravity and therefore the fluid is weightless, and no signals are sent. Yet the brain needs these signals for orientation. Without them, vertigo and the other symptoms of motion sickness occur. In moving cars and ships, the fluids slosh around so that the brain receives chaotic and confusing signals, resulting in the same symptoms.
In a report in the March 16, 1901, issue of the
Journal of the American Medical Association,
Dr. Daniel R. Brower offered the following treatment plan: Before the trip one should "avoid excessive fatigue and mental worry," eat lightly, and produce a "free catharsis by means of a full dose of massa hydrargyri, followed at the proper time by a saline purgative." (What he meant by "full dose" and "proper time" was not explained.)
Once this cleansing of the bowels had been accomplished, he suggested adding one teaspoon each of "Potassii Bromidi" (potassium bromide) and "Aq. Menthae Piperitae" (mint or peppermint oil) to water and drinking it three times a day until boarding the ship. Once on board, one should then take 10 to 15 grains (1 grain equals approximately 65 milligrams) of "Chloralamid," lie down, and remain horizontal until the ship was at sea and the effects of the medication had worn off. (He did not comment on what these effects might be.) Then one should "move around on deck to ascertain whether he has obtained his 'sea legs.' " If the seasickness returns, the Chloralamid should be repeated. His last and probably best advice was to "remain on deck as much as possible."