Murder and Mayhem (3 page)
Authors: D P Lyle

A: We call this type of injury "blunt trauma," as opposed to "penetrating trauma" from a bullet or axe or other object. Blunt head trauma may result in anything from a simple bump on the head (contusion) to sudden death. The force of the blow alone may cause immediate loss of consciousness (concussion). To cause death, bleeding within or around the brain would most likely have to occur. This is called "intracranial bleeding." It may occur with
rupture of an artery, a vein, or multiple small capillaries in and around the brain. Concussions and intracranial bleeds can occur with or without a fracture of the skull.
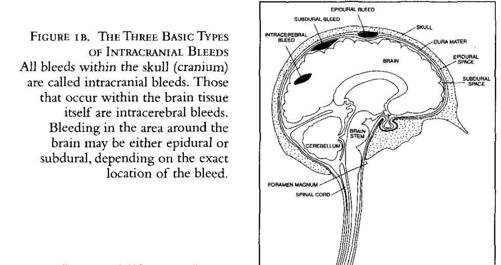
A membrane called the dura mater covers the brain. The space between the dura and the skull is called the epidural space, while the area between the dura and the brain is termed the subdural space (Figure 1a).
An intracranial bleed is one that occurs anywhere within the skull. They are of three basic types (Figure lb). Epidural and subdural bleeds occur in the space between the brain and the skull. Epidural bleeds are outside the dura mater and typically result from arterial bleeds from the epidural arteries, which are often torn by fractures of the skull. Subdural bleeds are usually venous in origin and occur in the subdural space. Intracerebral bleeds occur within the brain tissue itself. All are potentially lethal.
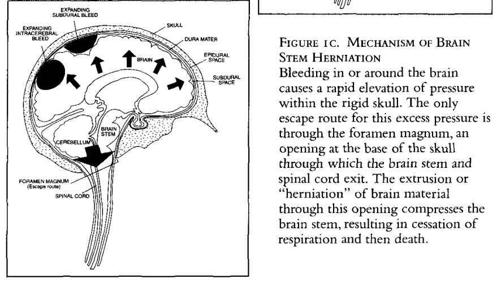
Remember, the skull is a rigid capsule that protects the brain. However, if bleeding occurs within the skull or within the brain itself, the bony skull cannot expand. Thus, pressure inside the enclosure rises rapidly, effectively "squeezing" the brain (Figure 1c).
At its posterior (toward the back) base (bottom), the brain narrows into a structure called the brain stem, which narrows further into the spinal cord, which in turn extends along the stack of bones called the spinal column down the back. The brain stem is a vital portion of the brain that, among other things, controls respiration.
The only outlet from the skull cavity is the hole (called the foramen magnum) at the base of the skull where the brain stem and spinal cord exit. It lies near the back juncture of the head and neck. The mounting pressure within the skull shuts down all brain function and ultimately pushes brain material into the foramen magnum and down along the brain stem and spinal cord. Think toothpaste tube. We call this "herniation of the brain stem." Not only is consciousness lost, but the compression of the brain stem also shuts down respiration; death follows in short order.

This process may occur over minutes, hours, or days. Remember how when you hit your head as a kid your mother would check you throughout the night to see if you were okay? That's because the bleeding may be slow, and headaches and coma and death may not occur for several hours. See, Mom was right.
Occasionally, people who have suffered blunt trauma do not develop any neurologic symptoms until days or weeks later. When headaches, nausea, blurred vision, numbness, or weakness in their extremities (all symptoms associated with rising intracranial pressure) occur, they visit a doctor, and a slow intracranial bleed is discovered.
The most likely injury in your situation would be a skull fracture with a rupture or tearing of an epidural artery (one of the many small arteries that course over the surface of the brain and are often torn with skull fractures), which would lead to bleeding. This would be classified as an epidural bleed. Arterial bleeding is usually brisk, and rising intracranial pressure, coma, apnea (loss of respiration), and death can occur very rapidly.
Most likely your victim would merely lie there, neither moving nor breathing. Such trauma could trigger seizure activity, though usually not, and that wouldn't fit your scenario anyway. When the heroine sees him immediately after the event, he may appear as if he is merely asleep. With a skull fracture a trickle of blood may appear from the ear or nose or both. Also, he may have a blue-black swelling (contusion) at the point of impact. Or there may be no external signs of injury.
A half hour later he would look . . . dead: blue-gray skin, flaccid (limp) limbs, dilated black pupils, no breathing, no pulse. The paramedics would most likely institute CPR and transport the victim to a hospital, where an M.D. would make the death pronouncement.
Can My Heroine Survive an Auto Accident and Ruptured Spleen?
Q: My sleuth is forced at gunpoint to drive to a remote area where she is certain she will be murdered. Her kidnapper, another woman, is riding in the passenger seat. They are traveling on a road temporarily closed for resurfacing. As they pass a few pieces of parked road equipment, my sleuth, desperate to save herself, spots a heavy-equipment trailer and veers into it at 30 miles per hour, hoping to selectively destroy the passenger side of the car. The steel trailer's rear bumper peels away the car's roof like the lid from a can, decapitating her tormentor. My heroine survives but is trapped with both shoulders broken and waits a half hour before being rescued. Later at the hospital we learn she has an injured spleen and is teetering between life and death. Needless to say, she is alive and beginning her long recovery by morning. Is my explanation way off the mark?
A: A ruptured spleen fits this scenario perfectly. Blunt trauma in a car accident, which is likely from a steering wheel injury, often results in a splenic rupture. It is very common in motorcycle accidents, football and skateboarding injuries, and so forth.
The spleen is a vascular organ (has a lot of blood in it); it sits in the left upper abdomen, tucked behind the lower margins of the ribs (Figure 2). It receives its blood from the splenic artery, a fairly large blood vessel. The spleen has a thin capsule that encases the soft and spongy splenic tissue (think blood-soaked sponge); thus it can rupture like a melon. In fact, its capsule is very easy to rupture or tear, and when breached, it will bleed profusely. During abdominal surgical procedures the spleen is handled with great care
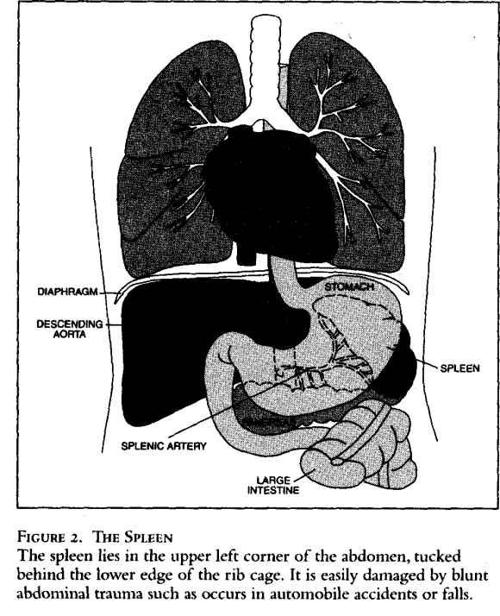
because even the delicate manipulations of the surgeon's fingers can injure it.
Although they can, people don't usually die from splenic ruptures. The reason? After enough blood is lost, the blood pressure (BP) drops, and the flow of blood into the splenic artery and the spleen lessens, the bleeding slows, and the process stops. The blood pressure of the injured person may go down to 60 or 70, but he or she can survive for a while in this degree of shock. The classic example of a splenic rupture is the teenager who slams his motorbike into a tree or car and arrives at the ER awake but lethargic with a BP of 70. Interestingly, once the victim is given blood and fluids and the BP begins to rise, the bleeding worsens—higher BP,
more blood into the spleen, more bleeding. Emergency surgery is the definitive treatment.
Of course, with your character stuck in the sitting position, gravity will hasten and magnify the degree of BP drop and the resulting shock syndrome. Still, she should survive the incident unless medical care is delayed too long.
Your character could exhibit several different symptoms as she waits for help and slips deeper into shock. Besides the pain in her damaged shoulders and abdomen, as the BP drops and shock sets in, your character will develop some or all of the following symptoms: dizziness, confusion, disorientation, hallucinations, nausea, vomiting, chills, shivering, thirst, cold sweats, blurred vision, sleepiness, weakness, a heavy feeling in her neck and extremities, and, finally, sleep or coma. Her reflection in the rearview mirror would be pale, even ghostly white, and maybe with a cyanotic tint (blue-gray hue due to shock and low blood oxygen levels). She may be in and out of consciousness or perhaps have vivid remembrances of things past akin to waking dreams.
Once rescued she will need immediate IV fluids, blood, and surgery to remove the spleen (splenectomy). Injured spleens are rarely repaired and almost always removed, since the spongy nature of the splenic tissue makes it very difficult to "fix." Besides, the spleen is not a vital organ, and people tend to get along quite well without one.
She should recover completely from the splenic rupture and splenectomy, and were this her only injury, she would be out of bed in a couple of days, home in a week, and back to normal by six weeks. However, recovery from her shoulder injuries, which could require surgical repair, would take a few months. The shoulder surgery would likely be delayed for several days after the splenectomy so she could be stabilized and prepared for this procedure. Before and after the surgery, the shoulders would be immobilized by placing her arms in slings, and she would require sedation and analgesic medications for the pain.
Where Can My Hero Be Shot and Survive?
Q: In my story the protagonist is shot. Obviously, he survives, but he is partially incapacitated. He must overcome the antagonist in a hand-to-hand fight. Where could he be shot and still function?
A: First, let's look at what happens when someone suffers a gunshot wound (GSW in medical shorthand). Ask any emergency department physician, and he will tell you that killing someone with a gun is not that easy. For a GSW to be immediately lethal, it must disrupt brain and/or heart function. Thus, a direct shot to the brain or heart is usually deadly in very short order. Also, a GSW to the lungs or a major blood vessel, such as the aorta, could be lethal in a manner of minutes or hours. Additionally, GSWs to the head, chest, or abdomen are severely incapacitating and would probably not fit your story.
That said, I might point out the following:
Many GSWs to the head do not penetrate the skull and thus do little brain damage. If the bullet approaches from a shallow angle, it may bounce off the skull and exit into the air or burrow beneath the scalp. In this situation a GSW that appears to be deadly at first would cause little harm, and your protagonist would fight on.
A GSW to the chest likewise might not penetrate the chest cavity, but instead might glance off a rib or the sternum (breastbone). In this case no major organ damage would occur, and your hero could continue his pursuit. The bullet might fracture a rib, which would be very painful with any movement and with breathing, particularly if he has to chase the villain.