Read Pediatric Primary Care Case Studies Online
Authors: Catherine E. Burns,Beth Richardson,Cpnp Rn Dns Beth Richardson,Margaret Brady
Tags: #Medical, #Health Care Delivery, #Nursing, #Pediatric & Neonatal, #Pediatrics
Pediatric Primary Care Case Studies (46 page)

The first part of any thorough physical examination is to simply observe the patient. Get a feeling for the gestalt of this patient. Appreciate any abnormal physical, movement, or behavioral findings as you enter the room and begin to speak with the patient and parents. Is there any syndromic appearance to the patient? Is there evidence of an organic disease such as thyroid disease? Evaluate the pattern of speech and word selection for age appropriateness. Direct questions to the patient and observe the content of responses. Observe how the patient interacts during the interview and examination. Is restlessness, hyperkinetic behavior, or excessive talking present during the interview?
The clinician should perform a thorough physical examination for two reasons. First, one wants to exclude medical conditions from the differential diagnosis. Second, if treatment is necessary, one must be sure there is no underlying medical condition, such as a congenital heart defect or arrhythmia, that might preclude or alter pharmacologic intervention.
Hearing screening should be an initial part of the assessment process.
Jason’s physical examination and hearing screening are both normal in all aspects. No neurological, cardiac, sensory, or thyroid abnormalities are identified.
What testing should be done?

Testing falls into two broad and general categories during an ADHD workup: medical and psychological testing. Evaluations should be thorough, but judicious use of potentially expensive tests should be practiced. Order tests based on an adequate index of suspicion.
First, findings during the interview or physical examination might indicate laboratory tests or imaging studies are necessary. For example, if thyroid disease is suspected, then order thyroid function studies. Expensive imaging studies such as MRI or CT scans of the brain should be ordered only if there is a high index of suspicion for neuropathology because these studies do not diagnose or rule out ADHD.
Second, the clinician should administer a DSM-IV-TR–based ADHD screening tool such as the revised Conners’ Scales or the Vanderbilt assessment, each of which has teacher and parent versions. Scoring and interpretation of these screening tests is very simple and thoroughly explained in the assessment manual for each tool. Such ADHD rating scales for parents and teachers have been shown to
have an odds ratio of 3.0 (equivalent to a sensitivity and specificity greater than 94%) in studies differentiating children with ADHD from normal, age-matched community controls (Green, Wong, & Atkins, 1999).
Additionally, the clinician may want to refer the patient to a psychologist for an extensive evaluation and psychometric testing to rule out low IQ, psychiatric diagnoses, learning difficulties, or developmental problems as contributing factors or as the actual diagnosis. Ideally, when behavioral consultation appointments are scheduled, Conners’ Scales or Vanderbilt assessments should be sent to the parents and teachers for completion prior to the appointment. Include a preprinted instruction letter for teachers that requests additional written information she or he believes is important in the evaluation of the child. This allows more information to be discussed at the appointment and also, if indicated, pharmacologic treatment to immediately begin.
In this case, Conners’ Scales were completed by Jason’s parents and two teachers prior to the appointment. The results are significant for elevation in measures of hyperactivity-impulsivity and inattention by all four evaluators. The teachers scored Jason significantly higher on the hyperactivity-impulsivity scale than the parents did.
It is common to see children suspected of having ADHD score higher on the scales of hyperactivity-impulsivity and inattention in a structured setting. Often, the behaviors are less noticed or less problematic at home where activities are not as structured and the child is not required to follow group rules. There can be great variation between parental observations as well. Depending on how much time and under what circumstances a parent interacts with a child, this parent may not be exposed to the problem behaviors voiced by teachers and the other parent. It is not uncommon for divorced parents to claim completely different behaviors are observed when the child is in each household. Reviewing the results of these screening tests allows parents to see how their child compares to similar aged peers in the areas of attention and impulsivity from the viewpoint of several adults while the child is in different settings.
Making the Diagnosis
Based on the interview and information obtained from the Conners’ Scales, it appears that Jason meets the criteria for ADHD. His mother has indicated that she has reservations about her son being labeled with a psychiatric diagnosis and is concerned about medical management. Additionally, she explains that his father believes these behaviors are just a part of being a boy, although the father has agreed to a short trial of the medication because Jason is having academic difficulties. However, he remains skeptical about treating for a prolonged period of time. The mother asks how long Jason will be treated and what side effects they should expect to see with medication.
Management
What type of education should you provide to a family when treating a child diagnosed with ADHD?
It is extremely important to educate the parents and child about why ADHD is treated, what medications are used, and what follow-up care will be needed in the short term and long term. There is much confusion in the general population about the medications used to treat ADHD. This confusion often results from misinformation obtained through the news media, the Internet, or friends and family members. Clinicians must educate parents and patients about the expected results and potential side effects when treating ADHD with a prescription medication. Free information is available online for parents and clinicians from the American Academy of Pediatrics (
http://www.aap.org
), the American Academy of Child and Adolescent Psychiatry (
http://www.aacap.org
), and the organization Children and Adults with Attention Deficit/Hyperactivity Disorder (
http://www.chadd.org
). During the visit provide an overview of medications used to treat ADHD. Outline the categories of medications, how they work, and what side effects to expect.
The patient will need to be followed up by telephone and in person as the medication is titrated to an effective dose. Inform the parents about titrating the dose based upon the response in their child as an individual. Then, follow-up at various intervals to assess the efficacy of the medication over time. Follow-up visits provide an opportunity for the healthcare provider to assess the patient while giving parents and patients a voice in how the medication is titrated. This type of communication also lessens the likelihood of confusion leading to a medication being unnecessarily discontinued.
A caveat to remember is that if there is no observable change or minimal improvement seen when treating ADHD with medication at a therapeutic dose, then another medication should be considered. If two or more medications have been tried without success, then additional workup and consideration of other diagnoses is indicated. It is important to utilize evidence-based medicine practices when treating ADHD to assure the correct diagnosis is made and an effective treatment strategy is providing desired results (Epstein, Rabinar, & Johnson, 2007; Leslie, Weekerly, Plemmons, Landsvere, & Eastman, 2004).
What medication should be used in the first line of treatment of ADHD?
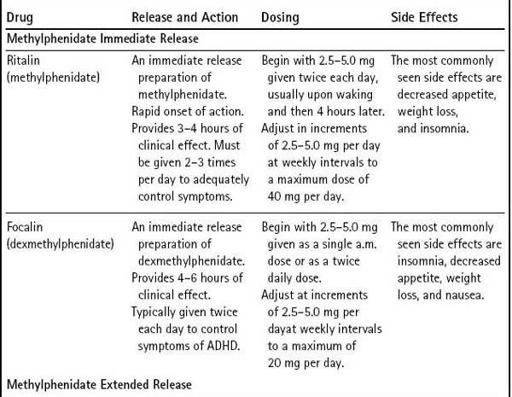
Two classes of FDA-approved medications are used as first-line treatment of ADHD in children and adolescents—stimulants and nonstimulants. The stimulants include the various methylphenidate and amphetamine products; the only approved nonstimulant is atomoxetine.
Table 12-3
lists these medications. Note that several medications are used off label for the treatment of ADHD. It is recommended that these medications be prescribed and monitored by a clinician who specializes in treating this disease. Therefore, these medications will not be discussed in this case study.
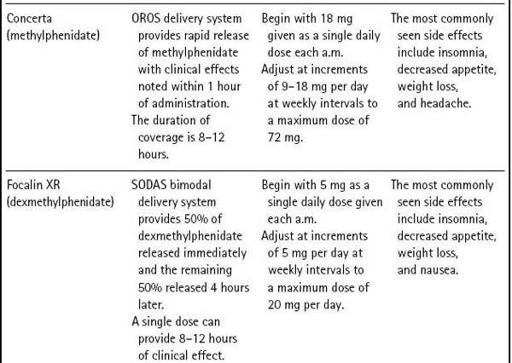
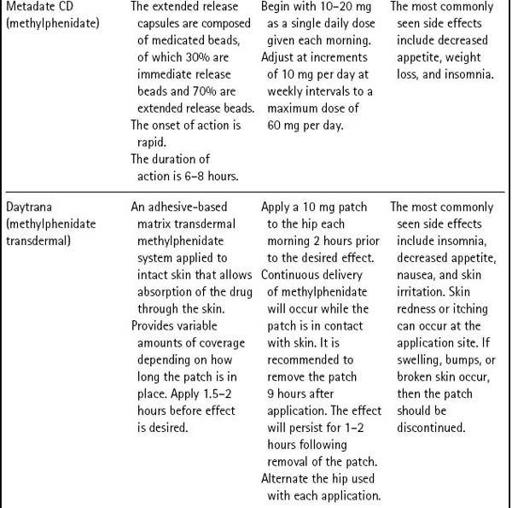
Table 12–3 Medications Approved to Treat ADHD in Children