Read Pediatric Primary Care Case Studies Online
Authors: Catherine E. Burns,Beth Richardson,Cpnp Rn Dns Beth Richardson,Margaret Brady
Tags: #Medical, #Health Care Delivery, #Nursing, #Pediatric & Neonatal, #Pediatrics
Pediatric Primary Care Case Studies (47 page)

Psychostimulants are the most frequently used medications for treating ADHD. Stimulants provide an effect in treating ADHD by blocking presynaptic reuptake of the neurotransmitters dopamine and norepinephrine and increasing the release of these monoamines into the synaptic cleft. With more neurotransmitter available at the synapse, signals are transmitted more efficiently. Atomoxetine blocks reuptake of norepinephrine, but does not significantly influence dopamine reuptake. Norepinephrine enhances relevant signals while dopamine suppresses irrelevant signals in the attentional areas of the brain.
Studies have shown that 80% of children treated with a stimulant medication have a good clinical response, with approximately 50% of those responders showing equivalent efficacy with methylphenidate or amphetamine, both of which have been used to treat attention problems for decades (Elia, Borcherding,
Rappoport, & Keysor, 1991; MTA Cooperative Group, 1999). It is important to realize that methylphenidate and amphetamine have different potencies. The typical conversion is 5 mg of amphetamine has potency equivalent to 10 mg of methylphenidate (Elia et al., 1991). Keep this in mind when changing from one of these products to the other.
Timing of Doses
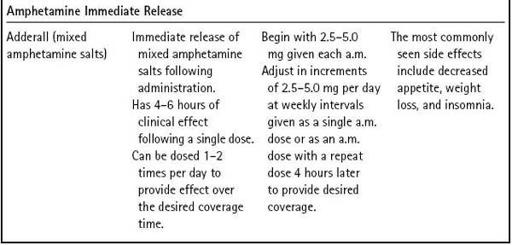
The immediate release forms of these drugs require multiple daily doses. Usually medication is given between 7:00 and 8:00 a.m. and again between 11:00 a.m. and 12:00 noon. Ideally, each dose results in 3–4 hours of positive clinical effect. The problem with immediate release formulations is that patients often have a window of subtherapeutic time prior to the next dose, during which symptoms return. This often occurs during the late morning at school or after school when homework needs to be completed. A third dose is sometimes given after school to allow patients to concentrate on homework. Multiple daily dosing becomes cumbersome for parents and teachers.
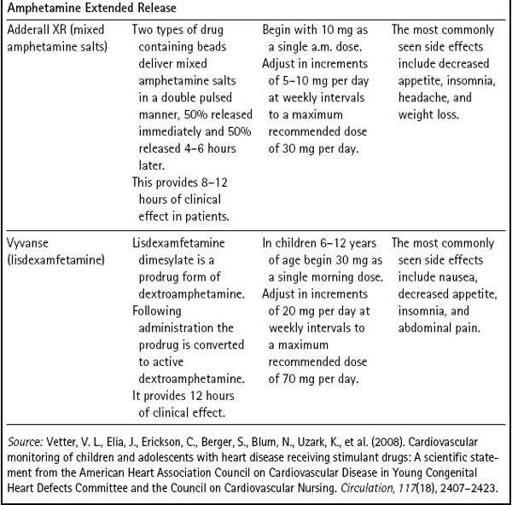
In the last decade, extended release formulations of methylphenidate and mixed amphetamine salts providing 8–12 hours of clinical effect following a single dose were introduced to the market. These medications revolutionized the treatment of ADHD with one dose per day providing extended control of symptoms. Studies show 8–12 hours of efficacy with a single morning dose. In 2006, a transdermal patch that delivers methylphenidate in an extended fashion was introduced to the market. Delivery through transdermal methylphenidate patches has allowed flexibility in treating ADHD over the waking day.
Atomoxetine is not a scheduled drug and has shown efficacy in reducing the symptoms of ADHD; it has safety and tolerability similar to that of methylphenidate (Michelson et al., 2002). It also may be given as a single daily dose. Decreased appetite and insomnia are side effects commonly seen in patients treated with atomoxetine (Wernicke & Kratochvil, 2002). Children and adolescents treated with atomoxetine were noted to have minor increases in diastolic blood pressure and heart rate, although there were no differences found on ECG tracings of patients treated with atomoxetine compared to those given placebo (Wernicke & Kratochvil). However, monitoring blood pressure and auscultating the heart should be a part of the routine examination.
A sample treatment plan is outlined in
Table 12-4
. Remember that feedback from the before-mentioned team is necessary before titrating these medications to their optimum dose. Poor communication between the clinician and parents should not be the reason a child receives less than optimal care for ADHD.
You suggest starting a long-acting medication each morning (5 mg of Focalin XR) and outline follow-up visits or interviews as listed in
Table 12-4
. The mother reiterates her concern about the safety of stimulant medications. In particular, she has read this class of medication can cause heart attacks and be fatal.
Table 12–4 Sample Treatment Approach for ADHD | |
| Type of Patient Interaction | Treatment Decisions to Consider |
| The diagnosis is established and treatment initiated at the first visit. | Education including proper dosing, onset of action, and potential side effects should be discussed prior to the first prescription being written. |
| A follow-up call from the parents following 1 week of treatment to check for efficacy, tolerability, and potential side effects. | Titrate to a higher dose if indicated. Reassure if typical side effects such as appetite decrease and trouble falling asleep are present. |
| A follow-up call from the parents following 1–2 additional weeks of treatment. | There should be some noticeable effect obvious to parents and/or teachers at this point. You must decide if an additional dosage increase is warranted now or wait until the next appointment. |
| 1 month in office follow-up visit. Weight and blood pressure should be recorded. | Inquire about efficacy at home, in school, and in social situations. Discuss appetite and sleep. Titrate to a higher dose if indicated. |
| Routine medication checks or maintenance visits every 3–4 months. | It is important to monitor continued efficacy and adverse effects. In particular, appetite and weight gain must be followed over time. Medication should be discontinued if the patient loses ≥ 10% of his or her body weight. |
What specific information about potential adverse effects in this class of medication should be given to the mother?

Cardiac Problems
There has been concern of an association between sudden death and using stimulant medications (Gutgesell et al., 1999). The American Heart Association (AHA, 2008) released a statement recommending a screening ECG in all children prior to beginning treatment with a stimulant medication (Vetter, Elia, & Erickson, 2008) to rule out any conduction disturbance that could be exacerbated by taking a stimulant medication. The AHA statement has been met with skepticism in the medical community because it contradicts the evidence-based medicine recommendations of the American Academy of Child and Adolescent Psychiatry and the American Academy of Pediatrics (American Academy of Pediatrics, 2000; Pliszka & American Academy of Child and Adolescent Psychiatry, 2007). A policy statement from the AAP published in August 2008 states there is no evidence to demonstrate the likelihood of sudden death is
higher in children receiving medications for ADHD than in the general population. Also, the text of this policy statement notes it has not been shown that screening ECGs before starting stimulants have an appropriate balance of benefit, risk, and cost effectiveness for general use in identifying risk factors for sudden death (Perrin, Friedman, & Knilans, 2008).
Despite these warnings, stimulant medications are widely used and historically have a safe profile with regard to adverse events. Many studies have shown participants have no significant cardiac events when treated with a stimulant medication. An important point for parents and patients to understand is that some of the concern is over effects with no clinical significance. For example, a study of one extended release methylphenidate product showed a statistically significant increase in heart rate, systolic blood pressure, and diastolic blood pressure (Quinn, 2005). However, these values were not clinically significant, meaning the changes are not detrimental to otherwise healthy patients using such medications.
It is the obligation of practitioners to ensure that patients are at minimal or no risk when taking medications to treat the symptoms of ADHD. Therefore, prior to prescribing such medications, a thorough physical examination should be performed with emphasis on the cardiac portion of the examination including measuring the blood pressure. Additionally, blood pressure should be measured and the heart should be auscultated at each medication follow-up visit. Caution should be exercised when using stimulant medications in patients with any cardiac abnormality, whether the etiology is structural or is a problem with electrical conduction. In such patients, a cardiology consultation is recommended before initiating therapy.
An important part of treating patients with ADHD is spending time educating parents and patients about the much more likely side effects seen with stimulant medications. The most common side effects seen secondary to using stimulant medications are appetite suppression and insomnia (Efron, Friedrich, & Barker, 1997).
Appetite
Some authors suggest the appetite suppression subsides after 1–3 months of treatment; however, some children will have appetite suppression for the duration of treatment with a stimulant.
Sleep Disturbances
Insomnia is often present in children with ADHD. It can be a basic part of the disease or can be secondary to medications prescribed to control the symptoms of ADHD. A small number of children sleep better after medication is started. Other children will require a medication to help with sleep. The medical literature has scant information about using medications to enhance sleep in children with ADHD. Most clinicians do not want to treat children with sedative
hypnotics. Clinicians have a few options when the treatment of insomnia is necessary. Melatonin is used to treat circadian rhythm disturbances and will induce sleep in children with ADHD. It can be purchased over the counter without a prescription. Also, the central alpha agonist clonidine helps induce sleep and has a rapid onset of action; however, clonidine has a variable half-life and should be carefully titrated to avoid “morning hangover” or hypotension in children. Additionally, the antidepressant trazodone effectively induces sleep and is used in patients with ADHD who have insomnia. Consulting with a pediatrician or child psychiatrist experienced in managing insomnia may be the safest and most effective means of achieving good sleep hygiene in patients with ADHD.
Jason’s mother agrees that a medication trial is indicated for Jason at this point. Focalin XR (methylphenidate) is started at 5 mg 7:45 a.m. each morning.
First Management Evaluation Visit
The mother phones in 8 days later with a report that Jason seems to be less hyperkinetic at school and pays more attention in the early part of the morning. By 10:00 a.m., however, he is behaving in the typical restless manner.
What is the best treatment intervention at this time?