The Design of Everyday Things (30 page)
Read The Design of Everyday Things Online
Authors: Don Norman

      Â
â¢
 Â
Lack of annoyance.
Because these sounds will be heard frequently even in light traffic and continually in heavy traffic, they must not be annoying. Note the contrast with sirens, horns, and backup signals, all of which are intended to be aggressive warnings. Such sounds are deliberately unpleasant, but because they are infrequent and for relatively short duration, they are acceptable. The challenge faced by electric vehicle sounds is to alert and orient, not annoy.
      Â
â¢
 Â
Standardization versus individualization.
Standardization is necessary to ensure that all electric vehicle sounds can readily be interpreted. If they vary too much, novel sounds might confuse the listener. Individualization has two functions: safety and marketing. From a safety point of view, if there were many vehicles present on the street, individualization would allow vehicles to be tracked. This is especially important at crowded intersections. From a marketing point of view, individualization can ensure that each brand of electric vehicle has its own unique characteristic, perhaps matching the quality of the sound to the brand image.
Stand still on a street corner and listen carefully to the vehicles around you. Listen to the silent bicycles and to the artificial sounds of electric cars. Do the cars meet the criteria? After years of trying to make cars run more quietly, who would have thought that one day we would spend years of effort and tens of millions of dollars to add sound?
 Most industrial accidents are caused by human error: estimates range between 75 and 95 percent. How is it that so many people are so incompetent? Answer: They aren't. It's a design problem.
Most industrial accidents are caused by human error: estimates range between 75 and 95 percent. How is it that so many people are so incompetent? Answer: They aren't. It's a design problem.
If the number of accidents blamed upon human error were 1 to 5 percent, I might believe that people were at fault. But when the percentage is so high, then clearly other factors must be involved. When something happens this frequently, there must be another underlying factor.
When a bridge collapses, we analyze the incident to find the causes of the collapse and reformulate the design rules to ensure that form of accident will never happen again. When we discover that electronic equipment is malfunctioning because it is responding to unavoidable electrical noise, we redesign the circuits to be more tolerant of the noise. But when an accident is thought to be caused by people, we blame them and then continue to do things just as we have always done.
Physical limitations are well understood by designers; mental limitations are greatly misunderstood. We should treat all failures in the same way: find the fundamental causes and redesign the system so that these can no longer lead to problems. We design
equipment that requires people to be fully alert and attentive for hours, or to remember archaic, confusing procedures even if they are only used infrequently, sometimes only once in a lifetime. We put people in boring environments with nothing to do for hours on end, until suddenly they must respond quickly and accurately. Or we subject them to complex, high-workload environments, where they are continually interrupted while having to do multiple tasks simultaneously. Then we wonder why there is failure.
Even worse is that when I talk to the designers and administrators of these systems, they admit that they too have nodded off while supposedly working. Some even admit to falling asleep for an instant while driving. They admit to turning the wrong stove burners on or off in their homes, and to other small but significant errors. Yet when their workers do this, they blame them for “human error.” And when employees or customers have similar issues, they are blamed for not following the directions properly, or for not being fully alert and attentive.
Understanding Why There Is Error
Error occurs for many reasons. The most common is in the nature of the tasks and procedures that require people to behave in unnatural waysâstaying alert for hours at a time, providing precise, accurate control specifications, all the while multitasking, doing several things at once, and subjected to multiple interfering activities. Interruptions are a common reason for error, not helped by designs and procedures that assume full, dedicated attention yet that do not make it easy to resume operations after an interruption. And finally, perhaps the worst culprit of all, is the attitude of people toward errors.
When an error causes a financial loss or, worse, leads to an injury or death, a special committee is convened to investigate the cause and, almost without fail, guilty people are found. The next step is to blame and punish them with a monetary fine, or by firing or jailing them. Sometimes a lesser punishment is proclaimed: make the guilty parties go through more training. Blame and punish; blame and train. The investigations and resulting punishments feel
good: “We caught the culprit.” But it doesn't cure the problem: the same error will occur over and over again. Instead, when an error happens, we should determine why, then redesign the product or the procedures being followed so that it will never occur again or, if it does, so that it will have minimal impact.
ROOT CAUSE ANALYSIS
Root cause analysis
is the name of the game: investigate the accident until the single, underlying cause is found. What this ought to mean is that when people have indeed made erroneous decisions or actions, we should determine what caused them to err. This is what root cause analysis ought to be about. Alas, all too often it stops once a person is found to have acted inappropriately.
Trying to find the cause of an accident sounds good but it is flawed for two reasons. First, most accidents do not have a single cause: there are usually multiple things that went wrong, multiple events that, had any one of them not occurred, would have prevented the accident. This is what James Reason, the noted British authority on human error, has called the “Swiss cheese model of accidents” (shown in
Figure 5.3
of this chapter on
page 208
, and discussed in more detail there).
Second, why does the root cause analysis stop as soon as a human error is found? If a machine stops working, we don't stop the analysis when we discover a broken part. Instead, we ask: “Why did the part break? Was it an inferior part? Were the required specifications too low? Did something apply too high a load on the part?” We keep asking questions until we are satisfied that we understand the reasons for the failure: then we set out to remedy them. We should do the same thing when we find human error: We should discover what led to the error. When root cause analysis discovers a human error in the chain, its work has just begun: now we apply the analysis to understand why the error occurred, and what can be done to prevent it.
One of the most sophisticated airplanes in the world is the US Air Force's F-22. However, it has been involved in a number of accidents, and pilots have complained that they suffered oxygen
deprivation (hypoxia). In 2010, a crash destroyed an F-22 and killed the pilot. The Air Force investigation board studied the incident and two years later, in 2012, released a report that blamed the accident on pilot error: “failure to recognize and initiate a timely dive recovery due to channelized attention, breakdown of visual scan and unrecognized spatial distortion.”
In 2013, the Inspector General's office of the US Department of Defense reviewed the Air Force's findings, disagreeing with the assessment. In my opinion, this time a proper root cause analysis was done. The Inspector General asked “why sudden incapacitation or unconsciousness was not considered a contributory factor.” The Air Force, to nobody's surprise, disagreed with the criticism. They argued that they had done a thorough review and that their conclusion “was supported by clear and convincing evidence.” Their only fault was that the report “could have been more clearly written.”
It is only slightly unfair to parody the two reports this way:
         Â
Air Force:
It was pilot errorâthe pilot failed to take corrective action.
         Â
Inspector General:
That's because the pilot was probably unconscious.
         Â
Air Force:
So you agree, the pilot failed to correct the problem.
THE FIVE WHYS
Root cause analysis is intended to determine the underlying cause of an incident, not the proximate cause. The Japanese have long followed a procedure for getting at root causes that they call the “Five Whys,” originally developed by Sakichi Toyoda and used by the Toyota Motor Company as part of the Toyota Production System for improving quality. Today it is widely deployed. Basically, it means that when searching for the reason, even after you have found one, do not stop: ask why that was the case. And then ask why again. Keep asking until you have uncovered the true underlying causes. Does it take exactly five? No, but calling the procedure “Five Whys” emphasizes the need to keep going even after a reason has been found. Consider how this might be applied to the analysis of the
F-22 crash:
Five Whys | |
Question | Answer |
Q1: Why did the plane crash? | Because it was in an uncontrolled dive. |
Q2: Why didn't the pilot recover from the dive? | Because the pilot failed to initiate a timely recovery. |
Q3: Why was that? | Because he might have been unconscious (or oxygen deprived). |
Q4: Why was that? | We don't know. We need to find out. |
Etc. | Â |
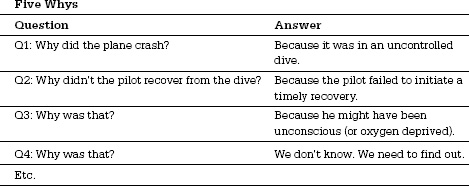
The Five Whys of this example are only a partial analysis. For example, we need to know why the plane was in a dive (the report explains this, but it is too technical to go into here; suffice it to say that it, too, suggests that the dive was related to a possible oxygen deprivation).
The Five Whys do not guarantee success. The question
why
is ambiguous and can lead to different answers by different investigators. There is still a tendency to stop too soon, perhaps when the limit of the investigator's understanding has been reached. It also tends to emphasize the need to find a single cause for an incident, whereas most complex events have multiple, complex causal factors. Nonetheless, it is a powerful technique.
The tendency to stop seeking reasons as soon as a human error has been found is widespread. I once reviewed a number of accidents in which highly trained workers at an electric utility company had been electrocuted when they contacted or came too close to the high-voltage lines they were servicing. All the investigating committees found the workers to be at fault, something even the workers (those who had survived) did not dispute. But when the committees were investigating the complex causes of the incidents, why did they stop once they found a human error? Why didn't they keep going to find out why the error had occurred, what circumstances had led to it, and then, why those circumstances had happened? The committees never went far enough to find the deeper, root causes of the accidents. Nor did they consider redesigning the systems and procedures to make the incidents
either impossible or far less likely. When people err, change the system so that type of error will be reduced or eliminated. When complete elimination is not possible, redesign to reduce the impact.