Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis (1124 page)
Authors: Mary A. Williamson Mt(ascp) Phd,L. Michael Snyder Md

BOOK: Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis
5.04Mb size Format: txt, pdf, ePub
Renin-producing tumors of the kidney
TABLE 16–66. Differentiation of Primary and Secondary Aldosteronism Based on Blood Tests and Clinical Symptoms
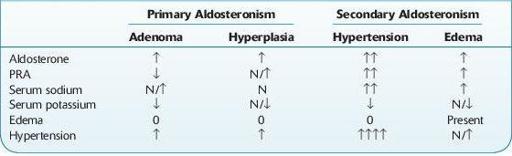
↑, increased; ↓, decreased; N, normal.
Decreased In
Other books
The Speed Queen by Stewart O'Nan
Flown By The Billionaire by Clara James
Worst Case Scenario - Book 5: Militia by G. Allen Mercer
Guide Me Home by Kim Vogel Sawyer
The Sworn by Gail Z. Martin
Emerald Embrace by Drake, Shannon
The Call of the Crown (Book 1) by T.J. Garrett
Cottonwood by Scott Phillips
Tied to the Tracks by Rosina Lippi