Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis (236 page)
Authors: Mary A. Williamson Mt(ascp) Phd,L. Michael Snyder Md

BOOK: Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis
6.3Mb size Format: txt, pdf, ePub
Cystine stones are rare, occurring in patients with homozygous congenital familial cystinuria, and characterized by bilateral obstructive staghorn calculi with associated renal failure.
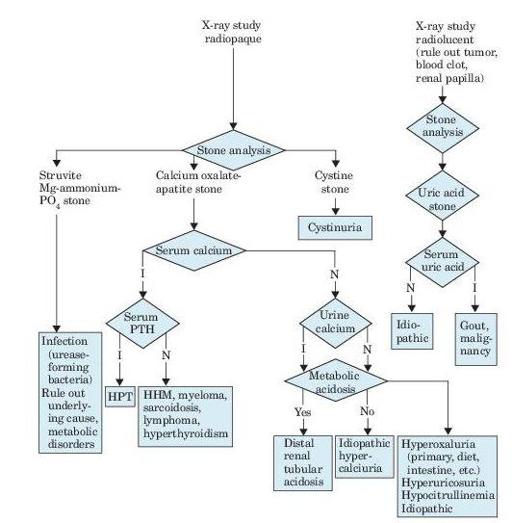
Figure 7–1
Algorithm for diagnosis of renal calculi, as revealed by flank pain, renal colic, hematuria, fever, and urinalysis findings. I, increased; N, normal; PTH, parathyroid hormone; HPT, hyperparathyroidism; HHM, humeral hypercalcemia of malignancy.
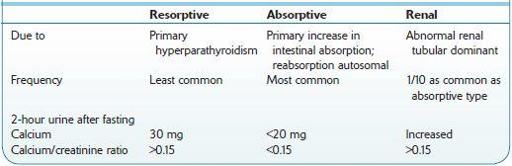
Table 7-1 Comparison of Types of Idiopathic Hypercalciuria
Who Should Be Suspected?
The waves or paroxysms of pain usually last 20–60 minutes and is related to the passage of the stone down the ureter and the associated ureteral spasm.
Other books
Undead and Unstable by Davidson, MaryJanice
Dimensions of Genesis by Q. Lee, Danielle
Unfinished Business (Erotic Reunion) - a SEXY romance short by Jordan, Lucia
Urban Necromancer by Chard, Phil
Little Criminals by Gene Kerrigan
Memnon by Oden, Scott
Edgar Allan Poe: The Fever Called Living (Icons) by Paul Collins
Daddy Cool by Donald Goines
Treason by Orson Scott Card
Hi-Tech Hijack by Dov Nardimon