The Zombie Combat Manual (24 page)
Read The Zombie Combat Manual Online
Authors: Roger Ma

The added difficulty of the situation is that after introducing the fundamental concept of death to a child, you then have to explain a phenomenon that flies directly in the face of that concept—the living dead. This is clearly not a simple conflict to explain. Children already have a difficult time understanding the permanent nature of death. Layer on top of that the possibility that the person they see die may
rise
from the dead, and you understand how complicated and confusing the explanation can become.
This is why many areas of developmental child psychiatry needed to be clearly delineated between the pre- and postzombie periods. An entirely new branch of treatment emerged to deal with this unique situation. We needed to rethink how we dealt with explaining concepts such as death, dying, and monsters to our young. As long as a child is old enough to understand the concept of life and death, he or she is old enough to understand the threat of the living dead.
This is why I recommend keeping it very simple. Explain the concepts as completely as possible, so that in the tragic case of the loss of a family member, the child understands that the person is permanently gone. Once this occurs, the deceased should be dealt with appropriately so as not to reanimate, or be immediately removed from the child’s field of vision. Without a doubt, the most difficult situation to manage is if a loved one passes and subsequently reanimates in front of the child. In these cases, the child needs to understand that it is no longer the same individual and poses a mortal threat. This becomes additionally complex when adults give a metaphysical explanation of death to their children. Saying something like “Daddy’s in heaven” can prompt the child’s question “Why did he choose heaven over us?” Seeing that person reanimate may be construed by the child as “Daddy changed his mind!” ending with the child running to embrace the reanimated individual. I’ve tried to address it as best as I could in my books, but I’m the first to admit that this is not an easy process. It’s why I still conduct seminars like this one today.
ZCM: How was your information received by the public?
JB:
We had our work cut out for us. Getting people to pay attention wasn’t easy. During large-scale infestations like the ones we were dealing with, this type of information is the last thing people want to think about. Medical crisis resource management teams were overwhelmed enough in dealing with the physical distresses of undead assault; the psychological response was often ignored or implemented too late. In areas where we were able to blitz the population with information, leaflets, and seminars, we saw dramatic decreases in child mortality rates, resulting both from the undead and from the living.
ZCM: What do you mean, “from the living”?
JB:
One of the tragic ancillary effects of an undead outbreak is a steep increase in family annihilations—in which one family member decides, for the sake of the household, that it is better to end the family’s existence by his hands than those of the living dead. I say “his hands” because traditionally annihilations are committed by a male family member. However, there are times when it is both parents committing the act together. Very sad, especially when you consider that children actually have a very high survival rate during outbreaks, even more so when taught by their parents how to protect themselves.
ZCM: Is that a fact?
JB:
It may be hard to believe, but it’s true. This is one thing that the public still doesn’t completely understand. Children are highly resilient beings, much more so than we give them credit for. Although it’s difficult for them to grasp the initial concepts, they are open to the idea of bogeymen that they need to avoid and escape from.
The other problem we faced was parents who waited too long to have these discussions with their children. Most believed that they would be able to protect their families, that they wouldn’t be infected, and as a result, they didn’t plan for the situation in which one or both of them were contaminated. This plays directly into the insidious nature of the infection. In our research, we meticulously analyzed the virus’ pathology in an attempt to decipher a pattern in the reanimation sequence. If we could find any consistencies in the time from death to reanimation, we could educate adults who wanted to wait until the last possible moment to say their good-byes. We wanted to give the public the specific amount of time after infection before “P&T”—passing and turning—so they could plan accordingly.
We looked at dozens of external factors—healthy or sick, overweight or thin, young or old. After analyzing data from countless infections, we could find no consistency between the degree of injury, speed of demise, and time of reanimation, and so we were never able to develop an accurate predictive model. A healthy woman in her midtwenties suffering from an infected scratch may P&T in ten minutes, whereas an obese, diabetic man in his forties with an entire knob of flesh taken out of his arm may linger for three days. The inconsistency frustrated us to no end, mostly because we knew that it would result in adults who waited too long to establish an arrangement for their children and inevitably reanimate with kids still in their care. We knew the best advice we could give is to tell parents to have a three-step strategy if they become infected: plan in advance, say your good-byes, send them on.
The flipside of this tragic coin is parents who are turned by their own reanimated children. There are thousands of recorded cases of this type of transmission occurring. What we could not determine is whether the infection was accidental, the result of a parent not realizing the child had turned, or an intentional transmission. There was not much we could do to influence this population. Adults know the consequences. Unfortunately, when it comes to their own children, some parents choose to ignore the signs, or don’t care.
ZCM: Does the age of the child factor into what you tell them?
JB: With infants, this is not an issue at all. You simply need to ensure that babies are well fed, well protected, and comforted as much as possible so that their cries do not reveal your position and make them vulnerable to attack. With colicky babies, there’s not much that can be done; the best you can do is ensure that you are not traveling on open terrain, as a baby’s wail has been shown to draw in living dead from up to a mile away. Although this can be a significant liability, having an infant among your group can also be an asset, as they seem to have the ability to detect approaching zombies from a distance much greater than adults. If a baby starts to stir and whine for no apparent reason, it is most likely that a reanimate is near.
As they grow to become toddlers, they still have a limited understanding of the permanency of death, but this is the point at which guardians need to introduce the idea that a reanimated human is a threat and should be avoided at all costs. As children get older, certainly beyond preschool age, they should have a full understanding of the danger the living dead pose to their well-being.
ZCM: Why did you decide to study one of the sanctioned undead self-defense systems?
JB:
I’m first and foremost a physician. But I’m not so much of a clinical academic that I don’t realize the value of knowing what it’s like in the field. Although my primary focus is the psychological care of those exposed to the living dead, physical defenses could not be ignored. To remain uneducated about such a key element to surviving in an outbreak would be bordering on malpractice in my eyes. In order to impart the greatest level of treatment to my patients, I needed not only to learn how to defend myself, but also to be able to teach it to others.
There is also no question that if you are safeguarding children, you must know how to eliminate a reanimate without a firearm. How do you think a six-month-old is going to react when a twelve-gauge round from a Remington 870 goes off next to his ear? How many other undead will be drawn to your location from a wailing child, upset by the deafening sound of gunfire and the choking smell of smokeless powder? It is inarguable: if you’re defending the welfare of children against the undead, it’s imperative to know how to defend yourself with a weapon that doesn’t fire ammunition.
ZCM: Should children be taught to fight the undead?
JB:
As much as I would like to encourage it, I can’t. Human children, even preteens, face a difficult task confronting even another reanimated child, much less an adult specimen. Children simply do not have the strength to deal a terminal blow to the undead skull. They are, however, very effective at evading an attacking corpse, which explains their high survivability rate.
The best defense that can be taught to children under age thirteen is how to escape and steer clear of a zombie’s grasp. Anyone with children knows how fast crawling infants can speed away from you. Given the specimen’s poor coordination, children often can escape by simply dropping to their hands and knees and quickly crawling away, before the reanimate can stoop down and launch an attack.
People begin quietly filing into the room. Some of the adults are alone. Others are leading or carrying children.
JB:
I’m sorry. We’re going to have to end it here.
Dr. Ballantine leaves the interview table. As I see her approach the attendees, the steely demeanor that I experienced during our meeting seems to soften as she draws closer to the group. She bends down to greet a young girl, who whispers something about keeping monsters away. The doctor’s face breaks into a warm, comforting grin, and while embracing the child, she says “Yes, I will.”
V.
COMBAT STRATEGIES AND TECHNIQUES
War is a brain-splattering, windpipe-splitting art.
—LORD BYRON
Now that you have primed your mind, your body, and your weapons, it is appropriate to discuss the methods to bring these components together to most effectively engage the walking dead in combat. For those who have never encountered an attacking cadaver, the techniques described in this section may seem vicious, brutal, perhaps even excessive and gratuitous. Let us be perfectly clear: Combat with a walking corpse is unlike any struggle that you have ever faced in your life. There exists no equivalent comparison in human combat. There are no knockouts, no submissions, no standing eight-counts. Confrontation with a zombie ends with only one of two possible outcomes—a neutralized ghoul or a devoured human.
Before we explore detailed strategies suitable for the various ranges of undead combat, it is important to discuss the unique dynamics that factor into your success or failure in a physical engagement with the living dead. Normal human combat follows a nonlinear progression of difficulty that depends on many external factors, including strength, size, and skill level of your opponent. Battling a walking corpse is a different matter. Though no encounter with a zombie should be deemed “easy,” the general degree of difficulty seems to be heavily influenced by the distance between combatants.
Dr. James Bane, an eminent clinical researcher in the field of undead combat, conducted a comprehensive study of human-versus-zombie conflict to specifically analyze the importance distance plays in survivability. Because of the predictable nature of a zombie’s combat tactics, Bane surmised that it was possible to accurately forecast the probability of any successful engagement regardless of the enemy, provided it was undead. A graph depicting one of his most significant findings is shown here:
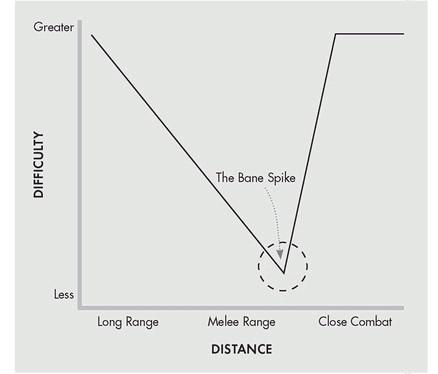
Bane discovered that long-range combat with the undead is most difficult because of the expertise and weaponry required. As the distance between combatants closes, this difficulty steadily decreases in direct proportion to the relative distance between opponents; the closer a zombie is, the easier it will be to dispatch. Eventually, the target enters what is considered the “sweet spot”—the optimal combination of distance, difficulty, and force required to successfully end the confrontation. Although this region will differ for each individual, this spot predominantly exists in the melee range of zombie combat, approximately three feet between combatants.
However, once a particular threshold has been crossed and the engagement evolves from a melee altercation into a close-combat encounter, the degree of difficulty skyrockets. The rise in difficulty is much steeper than earlier in the encounter and is nearly instantaneous. Bane determined that there are several reasons for this rapid transformation:
•
Fear:
The closer a zombie comes to its human prey, the more terrified that person may become when face-to-face with the attacker. This fear seems to be augmented if the ghoul has suffered grisly wounds and decay during its reanimated existence.