Fundamentals of Midwifery: A Textbook for Students (43 page)
Read Fundamentals of Midwifery: A Textbook for Students Online
Authors: Louise Lewis

BOOK: Fundamentals of Midwifery: A Textbook for Students
5.52Mb size Format: txt, pdf, ePub
A
traditional mother
(see Figure. 5.5): a woman who fulfils all three roles the genetic mother, gestational mother and the social mother.
traditional mother
(see Figure. 5.5): a woman who fulfils all three roles the genetic mother, gestational mother and the social mother.
A woman (the
commissioning mother
) who intends to raise a child carried by a surrogatemother (the gestational mother). She may also be the genetic mother, whose ovum was fertilised to become the embryo implanted in the womb of the gestational (surrogate) mother.
commissioning mother
) who intends to raise a child carried by a surrogatemother (the gestational mother). She may also be the genetic mother, whose ovum was fertilised to become the embryo implanted in the womb of the gestational (surrogate) mother.
A woman who legally takes on responsibility for the nurture of a child, through adoption,foster care, or a parental order, or alternatively, through marriage as a stepmother.The International Federation of Gynaecology and Obstetrics (FIGO) (2008) define surrogacy as:
. . . where a woman carries a pregnancy and delivers a child on behalf of a couple where the woman is unable to do so, because of congenital or acquired uterine abnormality or serious medical contraindication to pregnancy...
(FIGO 2008, p. 312)Brazier et al. (1998) define surrogacy as:
. . . the practice whereby one woman (the surrogate mother) becomes pregnant, carries and gives birth to a child for another person(s) (the commissioning couple) as the result of an
Sperm donorAdoptive father/ stepfather
 100
100
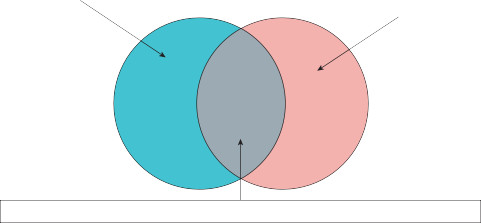 Genetic father (also the biological father)Traditional fatherSocial (commissioning) fatherIn some surrogacy arrangements the genetic father will also be the social father
Genetic father (also the biological father)Traditional fatherSocial (commissioning) fatherIn some surrogacy arrangements the genetic father will also be the social father
Figure 5.10
Venn diagram illustrating the nature of biological and social fatherhood (Ber 2000; Erin & Harris 1991; FIGO Committee for the Ethical Aspects of Human Reproduction and Women’s Health 2008).
agreement prior to conception that the child should be handed over to that person after birth . . .
(Brazier et al. 1998, Annexe A)The latter definition does not preclude commercial surrogacy arrangements for example. Brazier et al. (1998) further defined a surrogate mother as:
. . . The woman who carries and gives birth to the child . . . or ‘surrogate’. She may be the genetic mother (‘partial’ surrogacy) – i.e. using her own egg – or she may have an embryo
– which may be provided by the commissioning couple -implanted in her womb using in-vitro fertilisation (IVF) techniques...
(‘host’ or ‘full’ surrogacy [see Figure. 5.7]; Brazier et al. 1998, Annexe A)Adoptive mothers and foster mothers are more familiar variants of the social mothering role (see Figure 5.5) with whom midwives may also interact. The main difference is that a surrogacy arrangement is a contract, which is entered, prior to conception, for the benefit of the commis- sioning parents, whilst adoption and fostering are arrangements undertaken post-conception mainly for the benefit of the children (Wyatt 2009). Regardless of mode of conception, or iden- tity of the genetic parents, it is important that midwives grasp that UK law and the midwife’s sphere of practice recognises only the childbearing woman (gestational mother) as the mother during pregnancy and the postnatal period (ICM 2011 and NMC 2012. That is:
. . . the woman who is carrying or has carried a child as a result of the placing in her of an embryo or of sperm and eggs, and no other woman...
(Human Fertilisation and Embryology Act 2008)This is only superseded by the completion of a parental order, or through legal adoption (Griffith 2010). Parental orders take effect after six weeks postpartum; prior to this a surrogate mother may decide not to relinquish her baby (Human Fertilisation and Embryology Act 2008; Griffith 2010).Midwives normally rely on childbearing women to identify their babies’ fathers. Sometimes, none is identified. In the traditional model of families, or the nuclear family, the husband is both the genetic father and the social father (see Figure 5.10), where a:
. . . where a woman carries a pregnancy and delivers a child on behalf of a couple where the woman is unable to do so, because of congenital or acquired uterine abnormality or serious medical contraindication to pregnancy...
(FIGO 2008, p. 312)Brazier et al. (1998) define surrogacy as:
. . . the practice whereby one woman (the surrogate mother) becomes pregnant, carries and gives birth to a child for another person(s) (the commissioning couple) as the result of an
Sperm donorAdoptive father/ stepfather
100Genetic father (also the biological father)Traditional fatherSocial (commissioning) fatherIn some surrogacy arrangements the genetic father will also be the social fatherFigure 5.10
Venn diagram illustrating the nature of biological and social fatherhood (Ber 2000; Erin & Harris 1991; FIGO Committee for the Ethical Aspects of Human Reproduction and Women’s Health 2008).
agreement prior to conception that the child should be handed over to that person after birth . . .
(Brazier et al. 1998, Annexe A)The latter definition does not preclude commercial surrogacy arrangements for example. Brazier et al. (1998) further defined a surrogate mother as:
. . . The woman who carries and gives birth to the child . . . or ‘surrogate’. She may be the genetic mother (‘partial’ surrogacy) – i.e. using her own egg – or she may have an embryo
– which may be provided by the commissioning couple -implanted in her womb using in-vitro fertilisation (IVF) techniques...
(‘host’ or ‘full’ surrogacy [see Figure. 5.7]; Brazier et al. 1998, Annexe A)Adoptive mothers and foster mothers are more familiar variants of the social mothering role (see Figure 5.5) with whom midwives may also interact. The main difference is that a surrogacy arrangement is a contract, which is entered, prior to conception, for the benefit of the commis- sioning parents, whilst adoption and fostering are arrangements undertaken post-conception mainly for the benefit of the children (Wyatt 2009). Regardless of mode of conception, or iden- tity of the genetic parents, it is important that midwives grasp that UK law and the midwife’s sphere of practice recognises only the childbearing woman (gestational mother) as the mother during pregnancy and the postnatal period (ICM 2011 and NMC 2012. That is:
. . . the woman who is carrying or has carried a child as a result of the placing in her of an embryo or of sperm and eggs, and no other woman...
(Human Fertilisation and Embryology Act 2008)This is only superseded by the completion of a parental order, or through legal adoption (Griffith 2010). Parental orders take effect after six weeks postpartum; prior to this a surrogate mother may decide not to relinquish her baby (Human Fertilisation and Embryology Act 2008; Griffith 2010).Midwives normally rely on childbearing women to identify their babies’ fathers. Sometimes, none is identified. In the traditional model of families, or the nuclear family, the husband is both the genetic father and the social father (see Figure 5.10), where a:
Genetic father
is the man who provides the spermatozoon for fertilisation of the ovum.
is the man who provides the spermatozoon for fertilisation of the ovum.
Social father
is the man who provides nurture and care for the child following birth.The social father is a role shared by the traditional father, the commissioning father in a sur- rogacy arrangement, and also by stepfathers and adoptive fathers. The
traditional father
would have fulfilled both the social and biological roles.Illustrated in Figures 5.11 and 5.12 are some potential combinations of non-traditional fami- lies in which a midwife could be involved, via surrogacy arrangements.
 101
101
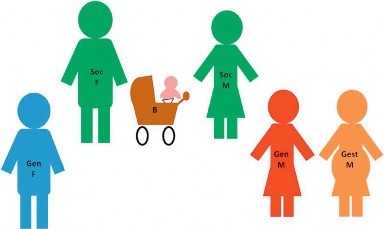 Gen F: Gen M: Soc F: Soc M: Gest M: B:
Gen F: Gen M: Soc F: Soc M: Gest M: B:
Genetic Father Genetic Mother Social Father Social Mother Gestational Mother Baby
Figure 5.11
A surrogacy arrangement with heterosexual commissioning parents who are not genetically related to the baby.
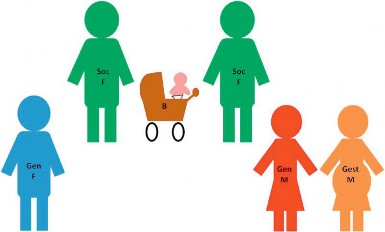 Gen F: Gen M: Soc F: Soc M: Gest M: B:
Gen F: Gen M: Soc F: Soc M: Gest M: B:
Genetic Father Genetic Mother Social Father Social Mother Gestational Mother Baby
Figure 5.12
A surrogacy arrangement with same-sex commissioning parents, neither of whom is genetically related to the baby.102
 Midwives must act as advocates for gestational mothers and their babies, remembering to ‘
Midwives must act as advocates for gestational mothers and their babies, remembering to ‘
. . . listen to the people in . . .
’ their ‘
. . . care and respond to their concerns and preferences
’ (NMC 2008, p. 3). However, they must negotiate and communicate sensitively with the family, as they choose to define themselves. Midwives are primarily concerned with supporting child- bearing women and babies whilst appreciating the diversity of parenting roles they may encounter.
Conception across the lifespan
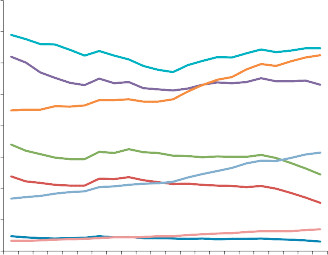
Parenthood may occur at different stages in a person’s lifespan. From a biological perspective,a woman may be no more than adolescent at first conception, or she may be on the cusp of menopause (Tiran 2008; Blackburn 2013). Men are also capable of fathering children from the time they reach sexual maturity; this effect is attenuated to a lesser extent with ageing in men, as many remain fertile well beyond the age of 40 (Ledger and Cheong 2011). The timing of conception may be controlled through the use of family planning and contraceptive strategies (see Chapter 12: ‘Contraception’, where family planning is discussed in greater depth), but also increasingly through assisted reproductive technology. Anxieties are often expressed about the health and welfare of women and their offspring when conception occurs in mothers at either extreme of the age spectrum for natural fertility. Midwives must be prepared to provide sensi- tive and supportive care for childbearing women across this age spectrum.Trends for conceptions by maternal age are pictured in Figure 5.13. The majority of concep- tions consistently occur in the 20–24 year age group, with the fewest being among women aged 40 years and over. For women, there are boundaries to their ‘
fertility
’ or ‘
fecundity
’. Women’s childbearing years begin, during puberty, with the development of secondary sexual charac- teristics, marked by the onset of hormonally regulated reproductive cycles, known as menarche.
Annual conception rate (conceptions per 1000 women)
160.0140.0120.0100.080.060.040.020.019901991199219931994199519961997199819992000200120022003200420052006200720082009201020110.0
 Under 16
Under 16
 Under 18
Under 18
 Under 20
Under 20
 20-24
20-24
 25-29
25-29
 30-34
30-34

is the man who provides nurture and care for the child following birth.The social father is a role shared by the traditional father, the commissioning father in a sur- rogacy arrangement, and also by stepfathers and adoptive fathers. The
traditional father
would have fulfilled both the social and biological roles.Illustrated in Figures 5.11 and 5.12 are some potential combinations of non-traditional fami- lies in which a midwife could be involved, via surrogacy arrangements.
101Gen F: Gen M: Soc F: Soc M: Gest M: B:Genetic Father Genetic Mother Social Father Social Mother Gestational Mother Baby
Figure 5.11
A surrogacy arrangement with heterosexual commissioning parents who are not genetically related to the baby.
Gen F: Gen M: Soc F: Soc M: Gest M: B:Genetic Father Genetic Mother Social Father Social Mother Gestational Mother Baby
Figure 5.12
A surrogacy arrangement with same-sex commissioning parents, neither of whom is genetically related to the baby.102
Midwives must act as advocates for gestational mothers and their babies, remembering to ‘. . . listen to the people in . . .
’ their ‘
. . . care and respond to their concerns and preferences
’ (NMC 2008, p. 3). However, they must negotiate and communicate sensitively with the family, as they choose to define themselves. Midwives are primarily concerned with supporting child- bearing women and babies whilst appreciating the diversity of parenting roles they may encounter.
Conception across the lifespan
Parenthood may occur at different stages in a person’s lifespan. From a biological perspective,a woman may be no more than adolescent at first conception, or she may be on the cusp of menopause (Tiran 2008; Blackburn 2013). Men are also capable of fathering children from the time they reach sexual maturity; this effect is attenuated to a lesser extent with ageing in men, as many remain fertile well beyond the age of 40 (Ledger and Cheong 2011). The timing of conception may be controlled through the use of family planning and contraceptive strategies (see Chapter 12: ‘Contraception’, where family planning is discussed in greater depth), but also increasingly through assisted reproductive technology. Anxieties are often expressed about the health and welfare of women and their offspring when conception occurs in mothers at either extreme of the age spectrum for natural fertility. Midwives must be prepared to provide sensi- tive and supportive care for childbearing women across this age spectrum.Trends for conceptions by maternal age are pictured in Figure 5.13. The majority of concep- tions consistently occur in the 20–24 year age group, with the fewest being among women aged 40 years and over. For women, there are boundaries to their ‘
fertility
’ or ‘
fecundity
’. Women’s childbearing years begin, during puberty, with the development of secondary sexual charac- teristics, marked by the onset of hormonally regulated reproductive cycles, known as menarche.
Annual conception rate (conceptions per 1000 women)
160.0140.0120.0100.080.060.040.020.019901991199219931994199519961997199819992000200120022003200420052006200720082009201020110.0
Under 16Under 18Under 2020-2425-2930-34Other books
The Abduction of Julia by Karen Hawkins
Fingerless Gloves by Nick Orsini
A Noble Captive by Michelle Styles
The Scold's Bridle by Minette Walters
The Cross and the Dragon by Rendfeld, Kim
Hue and Cry by Patricia Wentworth
Skulk by Rosie Best
Penpal by Auerbach, Dathan
The Keeper's Flame (A Pandoran Novel, #2) by Barbara Kloss