Examination Medicine: A Guide to Physician Training (94 page)
Read Examination Medicine: A Guide to Physician Training Online
Authors: Nicholas J. Talley,Simon O’connor
Tags: #Medical, #Internal Medicine, #Diagnosis

1.
syphilis
2.
diabetes mellitus
3.
alcoholic midbrain degeneration (rarely)
4.
other midbrain lesions.
SIGNS
1.
Small, irregular, unequal pupil.
2.
No reaction to light.
3.
Prompt reaction to accommodation.
4.
If tabes associated, decreased reflexes.
CAUSES OF PAPILLOEDEMA (
Fig 16.88a
)
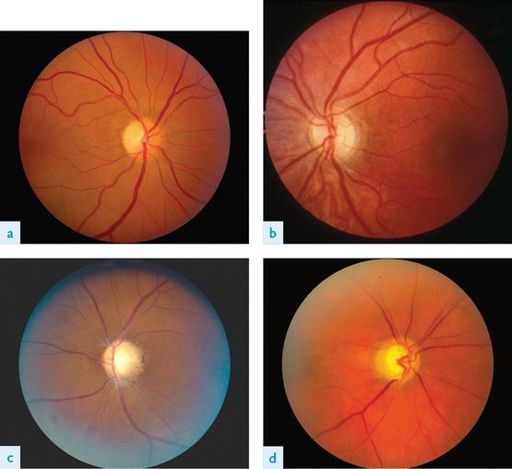
FIGURE 16.88
Patterns of optic atrophy. (a) Superotemporal sector atrophy in a 59-year-old woman with a supraclinoid internal carotid artery aneurysm compressing the optic nerve. (b) Band (‘bowtie’) atrophy in an 8-year-old boy with a craniopharyngioma compressing the optic chiasm. (c) Diffuse optic atrophy in a 41-year-old woman with neuromyelitis optica after a severe attack that left her with no light perception. (d) Glaucomatous cupping with atrophy of the superior and inferior neuroretinal rim appearing as ‘notching’ of the neuroretinal rim and vertical elongation of the cup. L A Levin, D M Albert (eds).
Ocular diseases: mechanisms and management
. Fig 44.1. Saunders, Elsevier, 2010, with permission.
1.
Space-occupying lesion (causing raised intracranial pressure) or a retro-orbital mass.
Table 16.50
Papilloedema versus papillitis
| PAPILLOEDEMA | PAPILLITIS |
| Optic disc swollen without venous pulsation | Optic disc swollen * |
| Acuity normal (early) | Acuity poor |
| Colour vision normal | Colour vision affected (particularly red desaturation) |
| Large blind spot | Large central scotoma |
| Peripheral constriction of visual fields | Pain on eye movement |
| Usually bilateral | Onset usually sudden and unilateral |
*
In retrobulbar neuritis and old papillitis the optic disc becomes pale.
2.
Hydrocephalus (associated with large ventricles):
a.
obstructive (block in the third ventricle, aqueduct or outlet to fourth ventricle – e.g. tumour)
b.
communicating:
c.
increased formation – choroid plexus papilloma
d.
decreased absorption – tumour causing venous compression, subarachnoid space obstruction from meningitis.
3.
Benign intracranial hypertension (pseudotumour cerebri, associated with small ventricles):
a.
idiopathic
b.
contraceptive pill
c.
Addison’s disease
d.
drugs – nitrofurantoin, tetracycline, vitamin A, steroids
e.
lateral sinus thrombosis
f.
head trauma.
4.
Hypertension (grade IV).
5.
Central retinal vein thrombosis.
6.
Cerebral venous sinus thrombosis.
7.
High cerebrospinal fluid protein level – Guillain-Barré syndrome.
CAUSES OF OPTIC ATROPHY (
Fig 16.88
)
1.
Chronic papilloedema or optic neuritis.
2.
Optic nerve pressure or division.
3.
Glaucoma.
4.
Ischaemia.
5.
Familial – retinitis pigmentosa, Leber’s disease, Friedreich’s ataxia.
CAUSES OF OPTIC NEUROPATHY
1.
Multiple sclerosis (see
Fig 12.1
).
2.
Toxic – ethambutol, chloroquine, nicotine, alcohol.
3.
Metabolic – vitamin B
12
deficiency.
4.
Ischaemia – diabetes mellitus, temporal arteritis, atheroma.
5.
Familial – Leber’s disease.
6.
Infective – infectious mononucleosis (glandular fever).
CAUSES OF CATARACT
1.
Old age (senile cataract).
2.
Endocrine – diabetes mellitus, steroids.
3.
Hereditary or congenital – dystrophia myotonica, Refsum’s disease.
4.
Ocular disease – glaucoma.
5.
Irradiation.
6.
Trauma.
CAUSES OF PTOSIS
1.
With normal pupils:
a.
senile ptosis (common)
b.
myotonic dystrophy
c.
fascioscapulohumeral dystrophy
d.
ocular myopathy e.g. mitochondial myopathy
e.
thyrotoxic myopathy
f.
myasthenia gravis
g.
botulism, snake bite
h.
congenital
i.
fatigue.
2.
With constricted pupils:
a.
Horner’s syndrome
b.
tabes dorsalis.
3.
With dilated pupils: third nerve lesion.
Third (oculomotor) nerve (p. 409)
HINT
When a patient has diplopia, ptosis and eye movement abnormalities not explained by cranial nerve problems, consider an ocular myopathy e.g. mitochondrial myopathy. Unlike myasthenia patients these do not worsen with repetition or maintenance.
CLINICAL FEATURES OF A THIRD NERVE PALSY (
Fig 16.89
)

FIGURE 16.89
Third nerve palsy. A 52-year-old woman with right upper lid ptosis from a third nerve palsy. Note the marked limited adduction and elevation of the right eye. The patient has less limitation to depression of the right eye. J A Nerad, K D Carter, M A Alford. Disorders of the eyelid: blepharoptosis and eyelid retraction. In
Rapid diagnosis in ophthalmology series: oculoplastic and reconstructive surgery
. Fig 5.6. Mosby, Elsevier, 2008, with permission.
1.
Complete ptosis (partial ptosis may occur with an incomplete lesion).
2.
Divergent strabismus (eye ‘down and out’).
3.
Dilated pupil unreactive to direct or consensual light and unreactive to accommodation.
HINT
Always exclude a fourth (trochlear) nerve lesion when a third nerve lesion is present. Do this by tilting the patient’s head to the same side as the lesion. The affected eye will intort if the fourth nerve is intact. Or ask the patient to look down and across to the opposite side from the lesion and look for intortion. Remember SIN:
Superior (oblique muscle), supplied by the IV nerve,
IN
torts the eye
AETIOLOGY
Central
1.
Vascular (e.g. brain stem infarction).
2.
Tumour.
3.
Demyelination (rare).
4.
Trauma.
5.
Idiopathic.
Peripheral
1.
Compressive lesions:
a.
aneurysm (usually on the posterior communicating artery)
b.
tumour causing raised intracranial pressure (dilated pupil occurs early)
c.
nasopharyngeal carcinoma
d.
orbital lesions – Tolosa-Hunt syndrome (superior orbital fissure syndrome – painful lesion of the third, fourth, sixth and the first division of the fifth cranial nerves)
e.
basal meningitis.
2.
Infarction – diabetes mellitus, arteritis (pupil is usually spared).
3.
Trauma.
4.
Cavernous sinus lesions.
Sixth (abducens) nerve (p. 409)
CLINICAL FEATURES OF A SIXTH NERVE PALSY
1.
Failure of lateral movement.
2.
Affected eye is deviated inwards in severe lesions.
3.
Diplopia – maximal on looking to the affected side; the images are horizontal and parallel to each other; the outermost image is from the affected eye and disappears on covering this eye (this image is also usually more blurred).
AETIOLOGY
Bilateral
1.
Trauma (head injury).
2.
Wernicke’s encephalopathy.
3.
Raised intracranial pressure.
4.
Mononeuritis multiplex.
Unilateral
1.
Central:
a.
vascular
b.
tumour
c.
Wernicke’s encephalopathy
d.
multiple sclerosis (rare).
2.
Peripheral:
a.
diabetes, other vascular lesions
b.
trauma
c.
idiopathic
d.
raised intracranial pressure.
HINT
1.
With the eye abducted: the elevator is the superior rectus (third nerve). The depressor is the inferior rectus (third nerve).
2.
With the eye adducted: the elevator is the inferior oblique (third nerve). The depressor is the superior oblique (fourth nerve).
CAUSES OF NYSTAGMUS
Jerky
1.
Horizontal:
a.
vestibular lesion (
Note:
Chronic lesions cause nystagmus to the side of the lesion – fast component.)
b.
cerebellar lesion (
Note:
Unilateral disease causes nystagmus to the side of the lesion.)
c.
internuclear ophthalmoplegia (
Fig 16.90
). (
Note:
Nystagmus is in the abducting eye, with failure of adduction on the affected side. This is a result of a medial longitudinal fasciculus lesion. The most common cause in young adults with bilateral involvement is multiple sclerosis; in the elderly, consider brain stem infarction. When the medial longitudinal fasciculus and the abducens nucleus on the same side are affected, the only horizontal movement the patient can make is abduction of the contralateral eye –
one-and-a-half syndrome
.)

FIGURE 16.90
Internuclear ophthalmoplegia. (a) Unilateral, gaze to the left (abnormal). (b) Bilateral, gaze to the right (abnormal). (c) Bilateral, gaze to the left (abnormal). (d) Bilateral, convergence (normal). A Compston, I McDonald, J Noseworthy et al. The symptoms and signs of multiple sclerosis. In
McAlpine’s multiple sclerosis
, 4th edn.
Fig 6.9
, Churchill Livingstone, Elsevier, 2006, with permission.